

One of the goals of the Affordable Care Act is to decrease readmission rates, which lead to wasting of resources and are associated with worse patient outcomes. While widely adhered to, there is no published research to support the practice of delaying discharge if the patient exhibits fever or hypothermia in the previous 24 hours. Our study quantifies the effect of abnormal body temperature before discharge on the readmission rate.
Methods:
Retrospective analysis of the minimal (Tmin) and maximal (Tmax) body temperatures during the last 24 hrs before discharge of all patients over 1 year period from our tertiary medical center were analyzed with T-test, ANOVA, uni-and multivariate logistic regression. Fever was defined as Tmax > 100.2F(2SDs from mean Tmax), hypothermia as Tmin < 96.7F(2SDs from mean Tmin).
Results: Descriptive analysis of the data from 19,038 inpatients are featured in Table 1 and Figure 1. The overall readmission rate was 10.2% (highest for General Medicine and Pediatrics); 4.7% of patients had an abnormal temperature 24 hrs before discharge; body temperature declined with age. ANOVA showed that 1st, the average number of days to readmission was not different between those with fever, hypothermia, and normothermia (mean+/-SD: 10.6+/-8.6; 12.1+/-8.6; 12.5+/-8.1, respectively); 2nd that the rate of readmission was not different between these groups, although there was trend for higher readmission among normothermic patients (2.9%; 0.3%; 7%, respectively). Table 2 features regression analyses that model readmission. Univariate analysis revealed that higher Tmax and age are associated with lower readmission probability. Both uni- and multivariate analysis showed that the presence of fever is associated with lower readmission probability and that compared with General Medicine, the other major primary services have lower readmission probability, when correcting for all the other listed variables.Table 1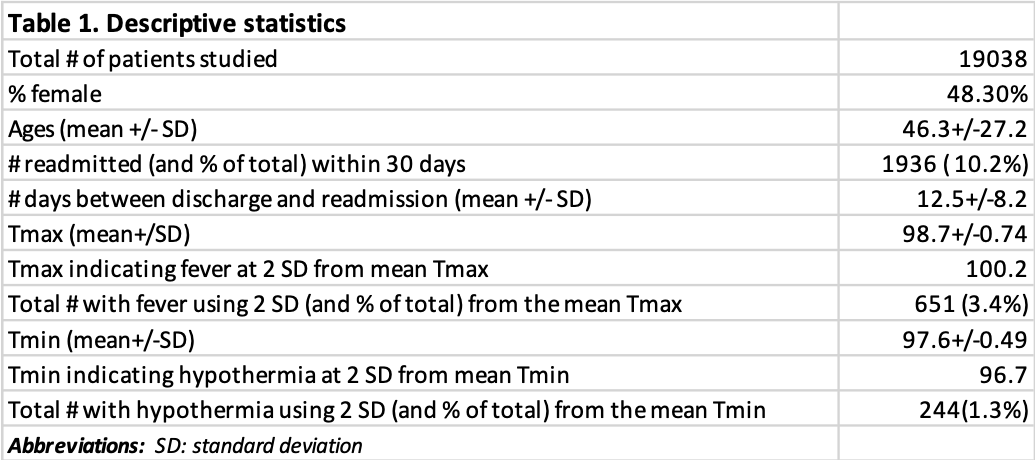 Figure 1
Figure 1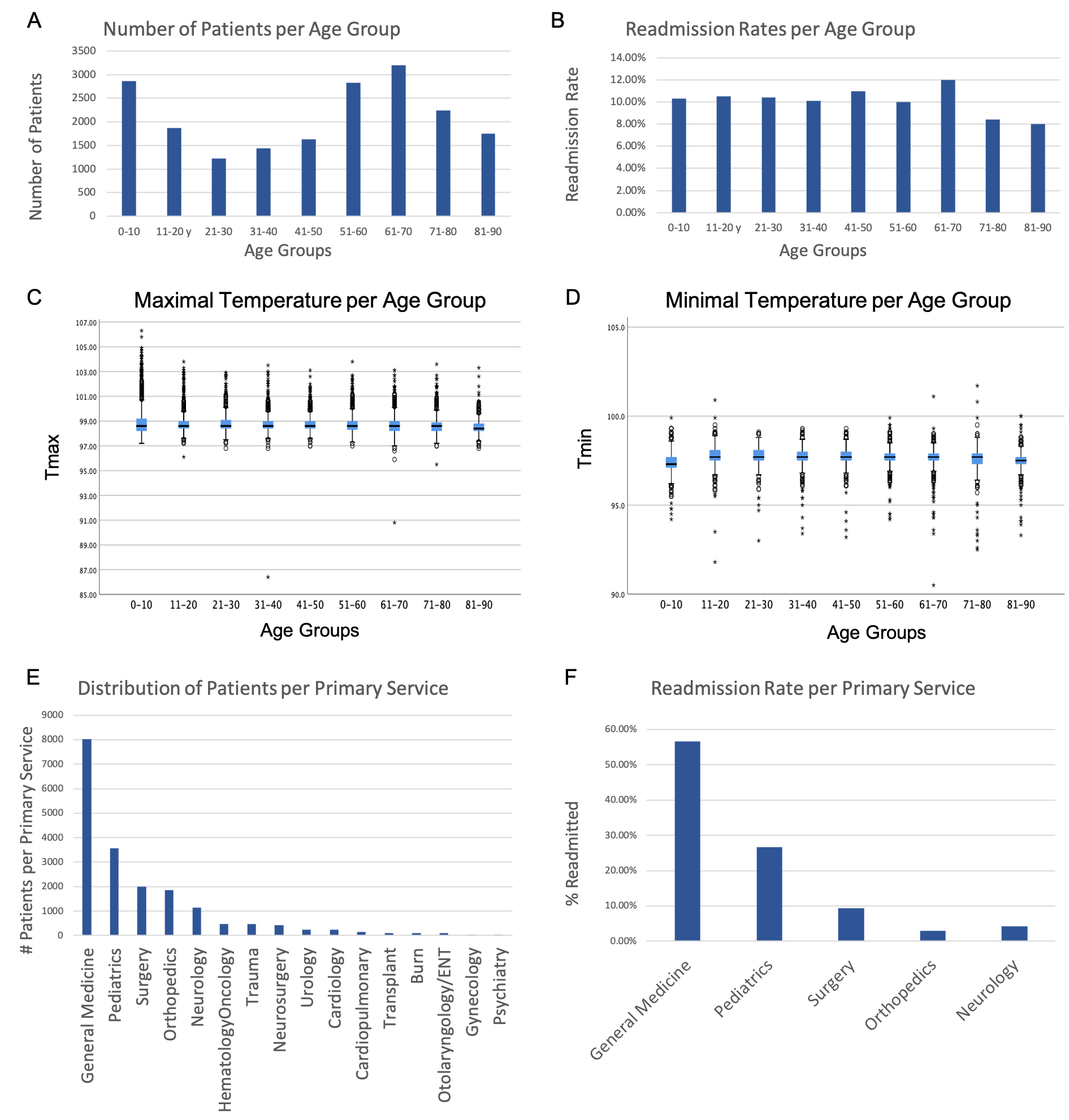 Table 2
Table 2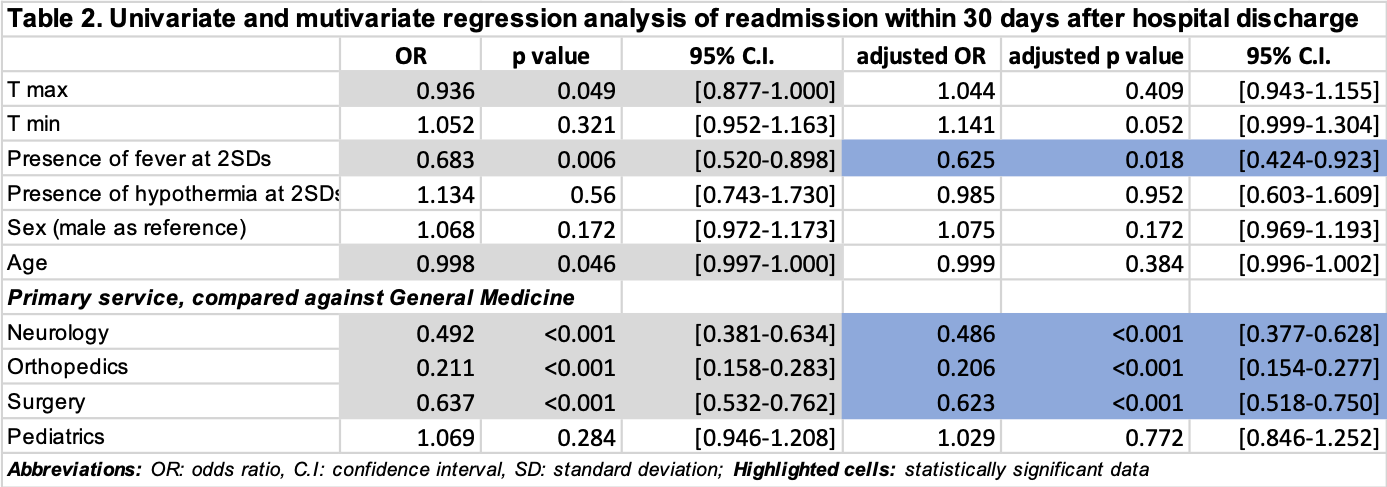
Conclusion: Our data clearly showed that abnormal body temperature measured within 24 hrs before discharge is not useful for predicting the chance for readmission. Therefore, delaying patients’ discharge based on Tmax or Tmin alone, taken outside the specific clinical context, may lead to wasting of hospital resources.

Ivayla I. Geneva, MD,PhD
Fellow
State University of New York Upstate
Syracuse, New York
Disclosure: I do not have any relevant financial / non-financial relationships with any proprietary interests.
Christina Lupone, MPH
Instructor
State University of New York Upstate
Syracuse, New York
Disclosure: I do not have any relevant financial / non-financial relationships with any proprietary interests.
Adam D. Wegman, BS
MD/PhD Student
State University of New York Upstate Medical University
Syracuse, New York
Disclosure: I do not have any relevant financial / non-financial relationships with any proprietary interests.
Kristopher M. Paolino, MD, MTM&H
Assistant Professor
State University of New York Upstate Medical University
Syracuse, New York
Disclosure: I do not have any relevant financial / non-financial relationships with any proprietary interests.
