Resident Physician University of Minnesota Minneapolis, Minnesota, United States
Introduction: Dural defects can arise spontaneously as natural history of certain pathologies. However, the relationship between dural defects and these certain pathologies has not been fully elucidated. Among the uncommon sequelae of dural defects are idiopathic thoracic spinal cord herniation- with less than 200 patients reported [1,2], intradural lumbar disc herniation (ILDH) comprising 0.04-0.33% of lumbar disc herniations [3,4], and idiopathic non-neurofibromatosis type dural ectasias [5].
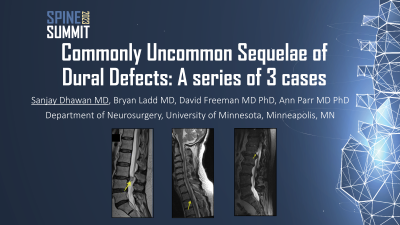
Methods: We reviewed clinical and radiological details for these three unique cases. Case I is a 60 year old male with sudden onset painless right foot drop and bilateral lower extremity hyperreflexia, weakness (Right&Left, proximal musculature 4/5, distal musculature 2/5) with a dural defect and spinal cord herniation noted at T2-T3 level.
Case II is a 65 year old female with acute onset bilateral lower extremity pain without- no any pertinent findings on neurologic examination, with intradural L3-L4 disc herniation with dural defect and annular tear that was identified intra-operatively.
Case III is a 63 year old male with gradually worsening right lower extremity weakness and atrophy, with focal dural defect at L1 level with erosion of posterior L1 vertebral body with nerve root entrapment.
Results: The imaging findings correlated well with the intraoperative findings for these three cases. For Case I, the dural defect was easily identified and the herniated spinal cord was reduced into the thecal sac with extra-dural reinforcement of the defect. For Case II, sequestered pieces of the disc were visualized intra-operatively. After durotomy, the disc fragments were found within the subarachnoid space and were removed. The patient reported improvement in pain in bilateral lower extremities post-operatively. Case III underwent posterior laminectomy at L1 with intradural repair of the dural defect. However, due to delay in diagnosis, the bone had regrown within the thecal sac, entrapping two nerve roots which were not salvageable.
Conclusion : Here we report often several examples of important sequelae of dural defects. A common 'etiology' is proposed here, with evidence supporting disc herniation as the primary cause of the dural defect, leading to these varied pathologies.