126 - Arteriovenous Fistula Salvage with the Minimally Invasive IRANI Procedure
Nicholas Kemper, BS – Medical Student, University of Louisville; Clinton Tyler, BS – Medical Student, University of Louisville; Bryan Glaenzer, MD – Assistant Professor, Interventional Radiology, University of Louisville
Purpose: Arteriovenous fistulae (AVF) are the preferred hemodialysis access modality due to increased durability, prolonged patency, and low infection rates. Notable disadvantages include a primary failure rate of up to 50%, prolonged maturation times, and significant abandonment rates. 46% of primary failure of AVF maturation is due to accessory veins creating alternate outflow routes. In accordance with the National Kidney Foundation 2003 Fistula First Breakthrough Initiative, avoidance of central venous catheter placement and salvage of these non-maturing fistulas is critical. We utilize the “IRANI” procedure, which involves tunneling needles deep and superficial to the target vein to serve as conduits for sutures which are then tied to occlude the accessory vein.
Material and Methods: Retrospective chart review investigating patient history, imaging, and interventional procedures performed in a single patient.
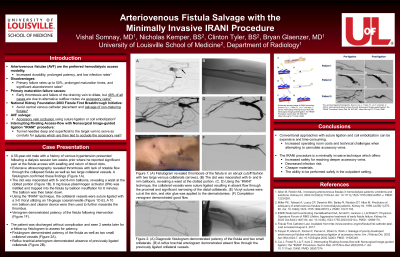
Results: A 55-year-old male with a history of venous hypertension presented following a dialysis session two weeks prior where he reported significant pain and swelling with return of blood clots at his access. Ultrasonography revealed occlusion of the fistula with two large collateral vessels. Fistulogram confirmed this finding. The clot was macerated with 6- and 8-mm balloons, revealing a waist at the clotted portion. 6 mg tissue plasminogen activator (tPA) was instilled and trapped into the fistula by balloon insufflation for 6 minutes. The balloon was then taken down. Using the “IRANI” technique, the collateral vessels were suture ligated with a 3-0 Vicryl utilizing an 18-gauge coaxial needle. A 10 mm balloon and cleaner device were then used to further macerate the thrombus. Venogram demonstrated patency of the fistula following intervention. The patient was discharged without complications. The fistula was patent at one-month follow-up.
Conclusions: The use of conventional approaches, such as surgical suture ligation and endovascular coil embolization, can be expensive and time-consuming due to increased operating room costs and technical challenges when attempting to cannulate accessory veins. The IRANI procedure utilized in our case is a minimally invasive technique which offers increased safety for reaching deeper accessory veins, decreased infection risk, cheaper materials, and the ability to be performed safely in the outpatient setting.