114 - Endovascular Intervention for Treatment of Acute Renal Vein Thrombosis Associated with Oral Contraceptives
Seema Al-Shaikhli, BS – Medical Student, Herbert Wertheim College of Medicine at Florida International University; Babitha Thatiparthi, MD – Radiology Resident, Larkin Community Hospital; Karolyna Rey, MD – Radiology Resident, Larkin Community Hospital; Kush Shah, MD – Interventional Radiologist, Larkin Community Hospital
Purpose: Renal vein thrombosis (RVT) is a rare condition, usually found in patients with nephrotic syndrome or renal malignancy. Less commonly, RVT can be observed secondary to oral contraceptive pill (OCP) use. Therefore, there are only a few reported cases in literature of OCP use as an identifiable risk factor for RVT. The purpose of this report is to describe a rare case of acute RVT associated with OCPs that was successfully treated with mechanical aspiration thrombectomy and lysis.
Material and Methods: A 30-year-old female with history of migraines and OCP use presented with sudden-onset, severe left-sided abdominal pain with radiation to the left flank. She recently discontinued her OCP a few days before her symptom onset. CT angiogram revealed edematous left kidney with non-opacified dilated left renal vein and an anatomical variant of a circumaortic left renal vein, confirming the suspicion of RVT. Intravenous heparin was started, but the patient was offered mechanical thrombectomy given persistent pain and worsening acute kidney injury in the setting of complete venous obstruction on repeated imaging.
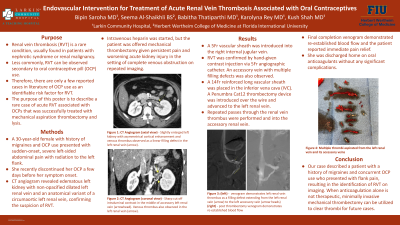
Results: A 5Fr vascular sheath was introduced into the right internal jugular vein. RVT was confirmed by hand-given contrast injection via 5Fr angiographic catheter. An accessory vein with multiple filling defects was also observed. Subsequently, an 14Fr reinforced long vascular sheath was placed in the inferior vena cava (IVC). A Penumbra Cat12 thrombectomy device (Penumbra Inc., Alameda, CA) was introduced over the wire and advanced to the left renal vein. Repeated passes through the renal vein thrombus were performed and into the accessory renal vein. Final completion venogram demonstrated re-established blood flow and the patient reported immediate pain relief. She was discharged home on oral anticoagulants without any significant complications.
Conclusions: Overall, our case described a patient with a history of migraines and concurrent OCP use who presented with flank pain, resulting in the identification of RVT on imaging. Similar to our case, when anticoagulation alone is not therapeutic, minimally invasive mechanical thrombectomy can be utilized to clear thrombi for future cases.