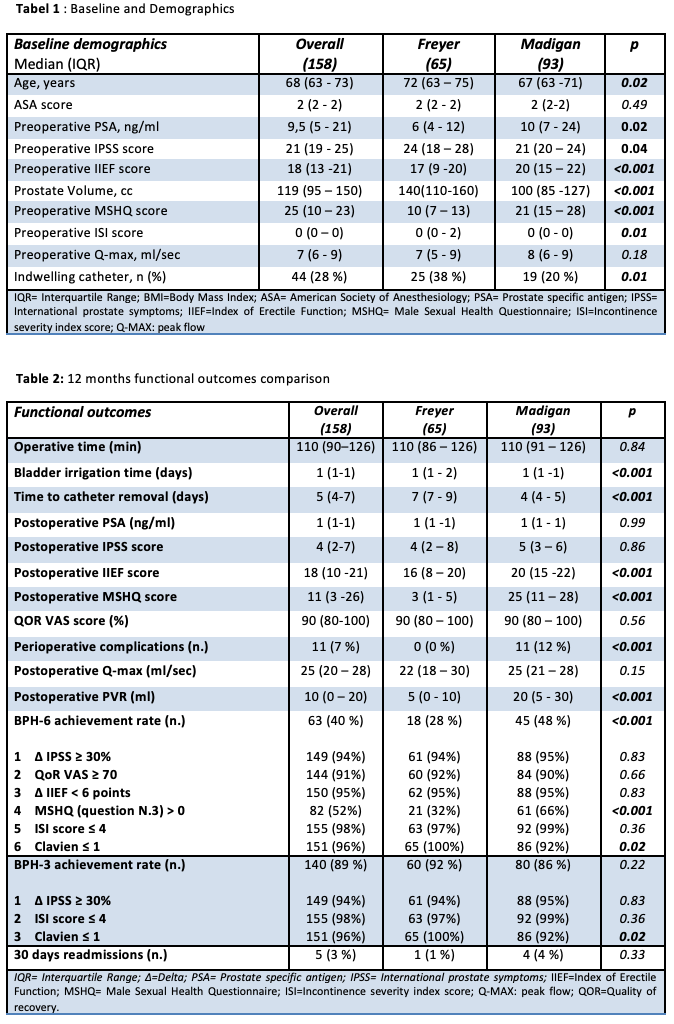
Introduction: BPH6 is a comprehensive metric to assess outcomes after treatment for BPO. Since the BPH6 includes: reduction of <6 points in International Index of Erectile Function (IIEF) and persistence of antegrade ejaculation at Male Sexual Health Questionnaire (MSHQ), only a small percentage of disobstructive procedures can lead to its achievement. We tested our novel BPH3 trifecta, in assessing the disobstructive proficiency of RASP according to different techniques. Methods: Baseline prostate volume (PV), flowmetry parameters and Validated questionnaires: IIEF, Incontinence severity index score (ISI), International prostatic symptoms score (IPSS), MSHQ, Quality of recovery (QOR), were recorded preoperatively and 12 months postoperatively. RASP were performed according to the urethra-sparing (Madigan) technique and a non urethra-sparing trans-vescical (Freyer) approach. The 2 cohorts were tested for our novel composite BPH-3 achievement rate as well as for BPH-6 achievement rate. BPH3 was defined as: ?IPSS=30%, ISI score =4, and No complications Clavien >1. Results: 158 patients underwent RASP (93 Madigan and 65 Freyer). Patients scheduled for Madigan procedure were younger, with lower PV, baseline IPSS score, overactive symptoms (ISI score), but higher MSHQ and IIEF score, when compared to the Freyer population (all p<0.02) (Table 1). At 12 months follow-up, Madigan patients reported a shorter bladder irrigation time and time to catheter removal (both p<0.001). A superiority in postoperative IEEF and MSHQ score were reported by the Madigan patients as expected (all p<0.001). Postoperative complication incidence was higher in the Madigan cohort, mainly due to UTI (p < 0.001). Although there were no differences in postoperative IPSS and Q-max between groups, the Madigan cohort presented with higher post void residue (p < 0.001) (Table 2). BPH6 achievement was higher in the Madigan cohort (48% vs 28%) (p < 0.001), while no difference was found in BPH3 achievement rate. Conclusions: Novel BPH3 composite trifecta appears to be more suitable than BPH6 in assessing the proficiency in disobstructive symptoms relief after RASP. SOURCE OF Funding: None