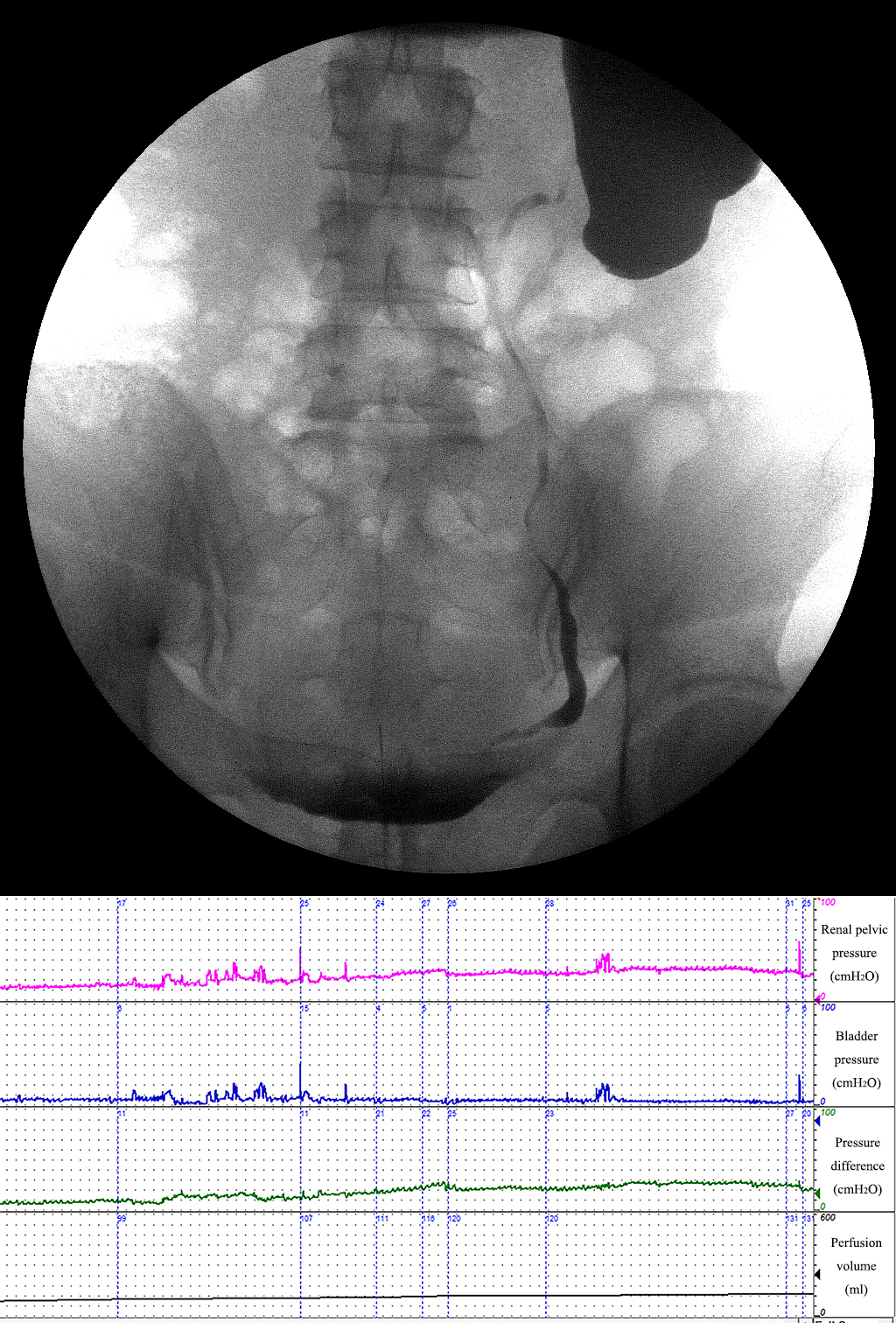
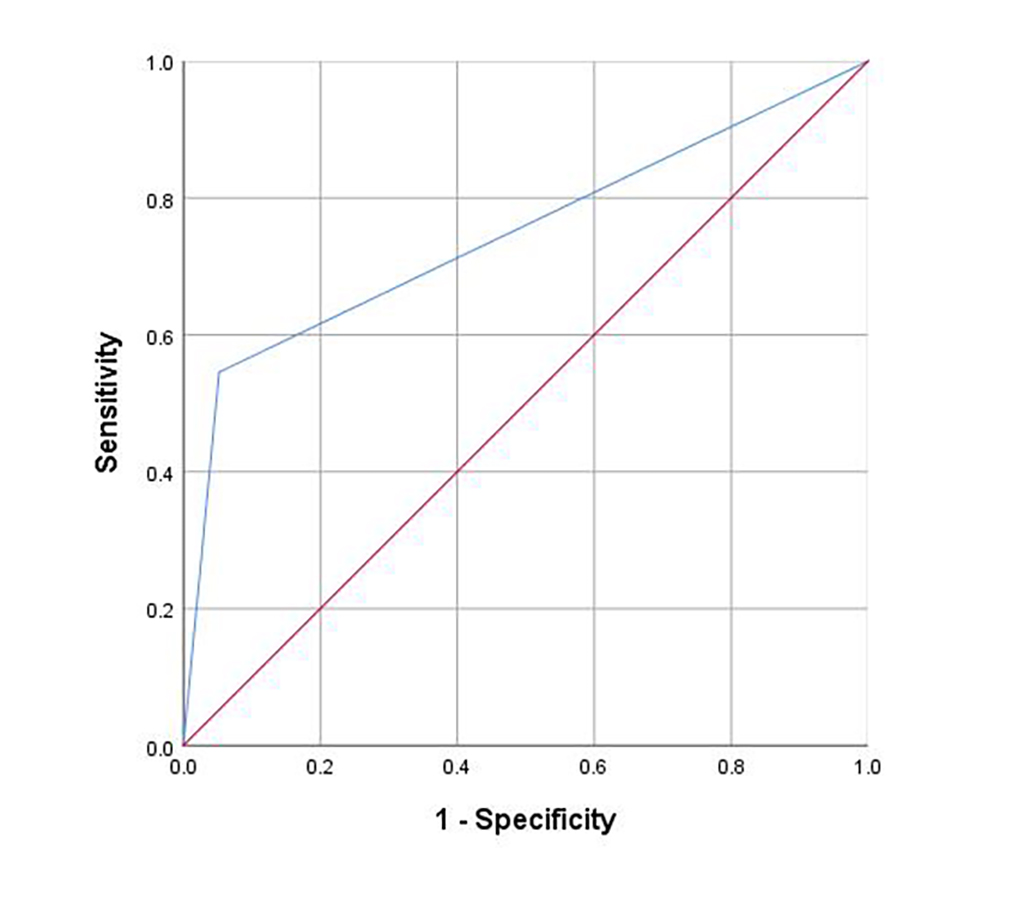
Introduction: To validate the modified upper urinary tract videourodynamics in reconstructed ureter with still dilation and hydronephrosis, and to explore the significance in guiding subsequent management. Methods: From December 2018 to November 2021, a total of 137 patients underwent upper urinary tract video urodynamics at the time of nephrostomy removal 3 months after the reconstruction. The urodynamic result was classified into 3 types. Type 1: the pressure remains stable near the baseline throughout the perfusion process, and the reconstructed ureter is well visualized. Type 2: The renal pelvic pressure increases with perfusion, while urography shows the ureteral peristalsis still exists. At the end of the examination, the pressure difference is lower than 15 cmH2O, and the renal pelvis pressure is lower than 22 cmH2O. Type 3: The renal pelvic pressure and pressure difference increase with perfusion and exceed the normal level. At the same time, ureteral peristalsis is weak or absent (Fig 1). Results: The patients were classified as type I in 124 cases, type II in 7 cases, and type III in 6 cases. All patients in type III received further treatment, including regular DJ stent replacement (2 cases), Allium stent (1 case), ureteroscopic balloon dilation (1 case), ureteroneocystostomy (1 case), and ileal ureter (1 case). Patients in type ? were instructed to avoid holding urine after the removal of nephrostomy and DJ stents. In 124 patients with type I, there was also 1 case receiving balloon dilatation and 4 cases replacing DJ tube. The sensitivity and specificity of the modified upper urinary tract videourodynamics in predicting the need for further treatment were 54.5% and 100% , and the area under curve was 0.747 (p=0.007) (Fig 2). Conclusions: The modified upper urinary tract videourodynamics can be used to evaluate the dilated upper urinary tract after reconstruction, and the classification has certain guiding significance for further treatment. SOURCE OF Funding: None.

.jpg "Xinfei Li, MD (he/him/his) photo")