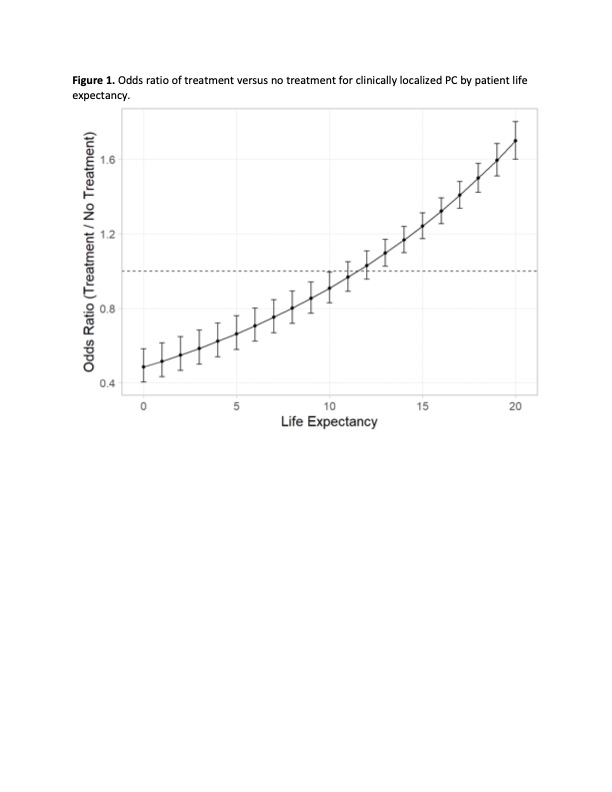
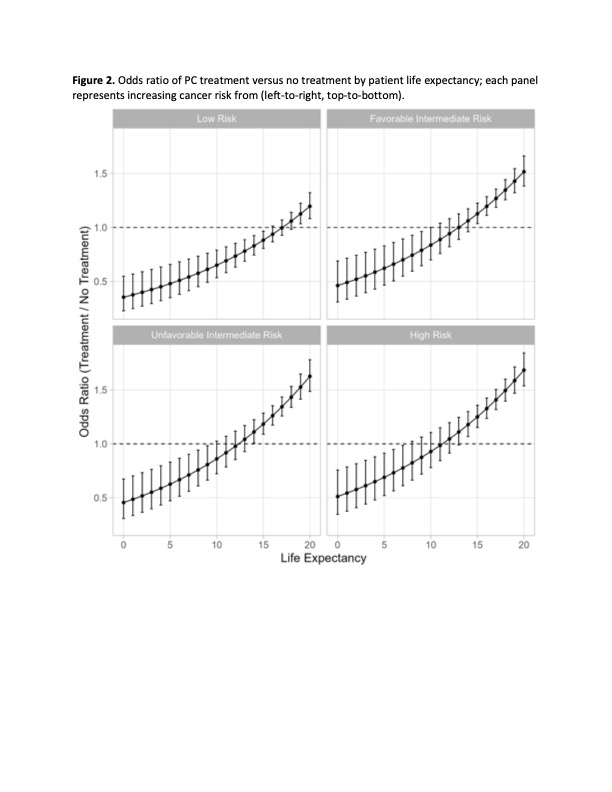
Introduction: Life expectancy (LE) thresholds for triage of treatment vs conservative management (CM) in prostate cancer (PC) guidelines are based on expert opinion. However, patient opinion of when to defer treatment based on LE is lacking. We crowdsourced a conjoint analysis to define at which LE men are more likely to choose against treatment. Methods: We used targeted crowdsourcing to query 2,046 men sociodemographically reflecting a US PC population based on SEER. We asked subjects to complete a conjoint analysis exercise in which they chose between treatment versus CM considering 4 tradeoffs: tumor risk, risk of erectile dysfunction, risk of urinary incontinence, risk of irritative urinary symptoms. Subjects were asked to consider LE throughout, which was calculated using the validated Prostate Cancer Comorbidity Index. Multinomial logistic regression defined the LE at which men were more likely to choose no treatment overall and in subgroups of tumor risk. Results: We found an interaction between LE and treatment, indicating the odds of treatment vs CM choice is dependent on LE (p < 0.001). The predicted probability of treatment decreased 15% with every 5 years of decreasing LE (OR 0.85, 95% CI .82-.89, p <0.001). Across all tumor risk levels, men were more likely to choose CM at a LE threshold <10 years (OR < 1, p < 0.05) (Figure 1). For low-, favorable intermediate-, unfavorable intermediate-, and high-risk cancers, men were more likely to choose CM at LE thresholds of <15, <10, <9, and <7 years, respectively. NCCN guidelines recommend CM overall at LE thresholds of £10 and <5–10 years for favorable and unfavorable intermediate-risk disease, and <5 years for high-risk disease (Figure 2). Conclusions: Patient preferences for LE cutoffs for when to consider CM align well with current guidelines recommendations, except for low-risk disease, for which patients are likely to consider conservative management even at LE <15 years, rather than <10. Guidelines should take patient preferences into account when recommending thresholds for CM. SOURCE OF Funding: .

 photo")