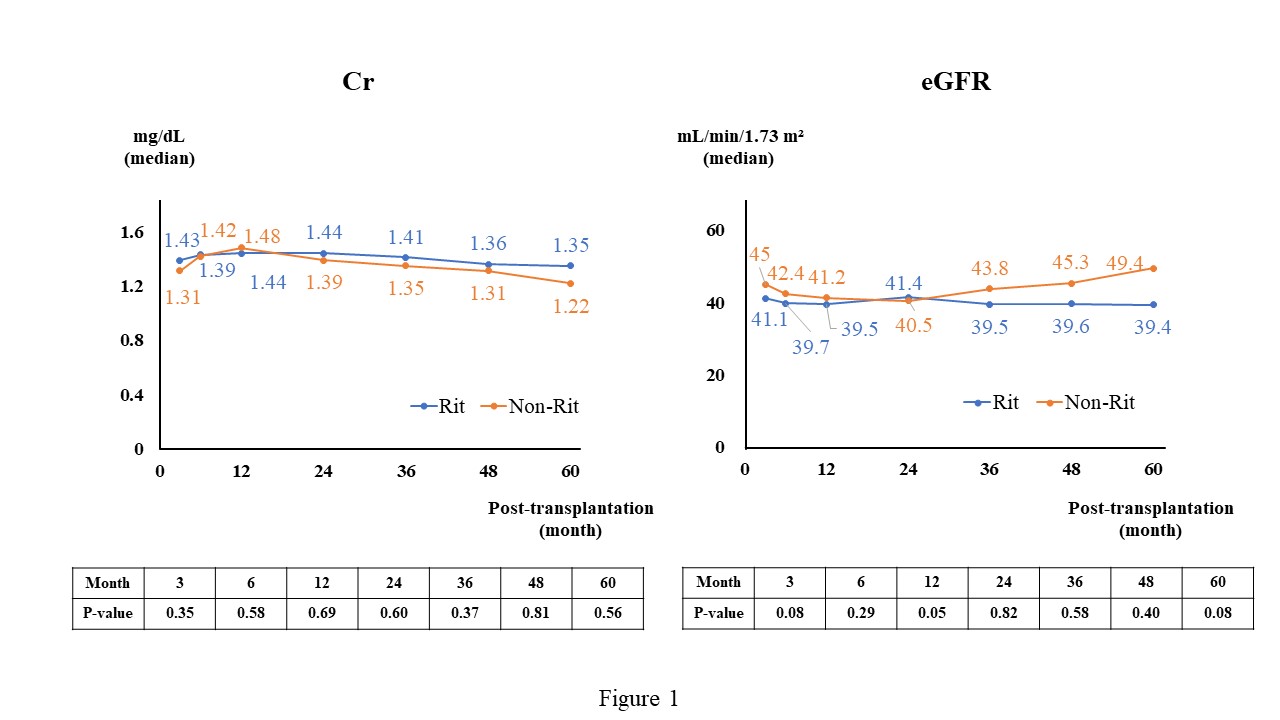
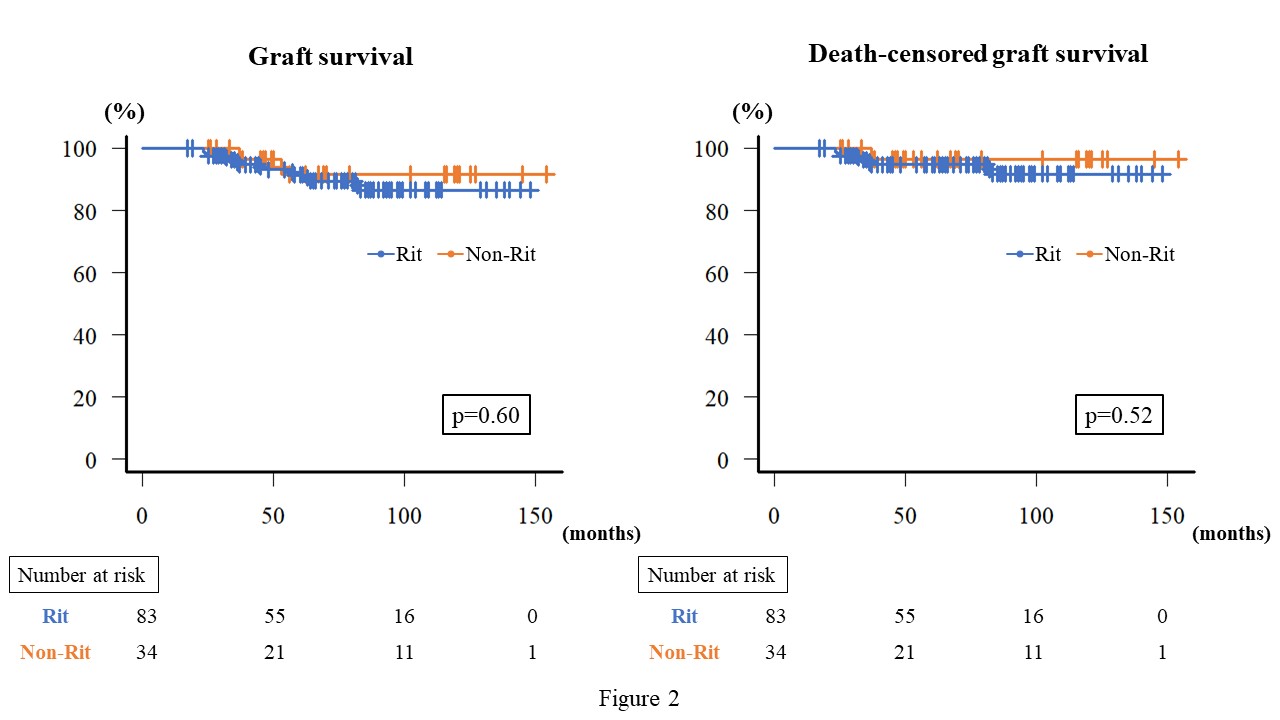
Introduction: We previously reported that low-dose rituximab induction therapy in immunologic high-risk patients for living donor renal transplantation did not increase CMV infections when preemptive therapy was performed. We now report additional long-term outcomes. Methods: One-hundred thirty-one recipients undergoing living-donor renal transplantation in our institution from May 2009 to September 2021 were evaluated retrospectively. Indications for preoperative rituximab (200 mg/body) were the following: 1. ABO major mismatch, 2. ABO minor mismatch, 3. donor-specific anti-human leukocyte antigen antibody (DSA)-positive, 4. Focal segmental glomerulosclerosis (FSGS). Results: There were 83 patients in the rituximab group and 34 in the non-rituximab group. Groups differed significantly in age (median age, 51 vs 42 years, respectively; P=0.03), but not in sex (male, 66% vs 68% P=1.00), FSGS (4% vs 0%, P=0.56). Estimated glomerular filtration rate did not differ significantly between groups until 5 years after transplantation (FIg.1). CMV clinical symptoms (14% vs 26%, P=0.18), including fever over 38 degrees (8% vs 12%, P=0.73) and gastrointestinal symptoms (7% vs 12%, P=0.06), and the 5-year survival rates of death-censored graft loss (95% vs 96%, P=0.52) did not differ significantly between two groups (Fig.2). Conclusions: As in our previous study, low-dose rituximab induction therapy was effective in immunologically high-risk recipients without increasing CMV infection without valganciclovir prophylaxis. Furthermore, the graft survival rate and renal function at 5 years after transplantation were equivalent to those in the non-rituximab group. SOURCE OF Funding: No