MP08-12: Sequential Intravesical Gemcitabine and Docetaxel for Treatment-Naive and Previously Treated Intermediate-Risk Non-Muscle Invasive Bladder Cancer
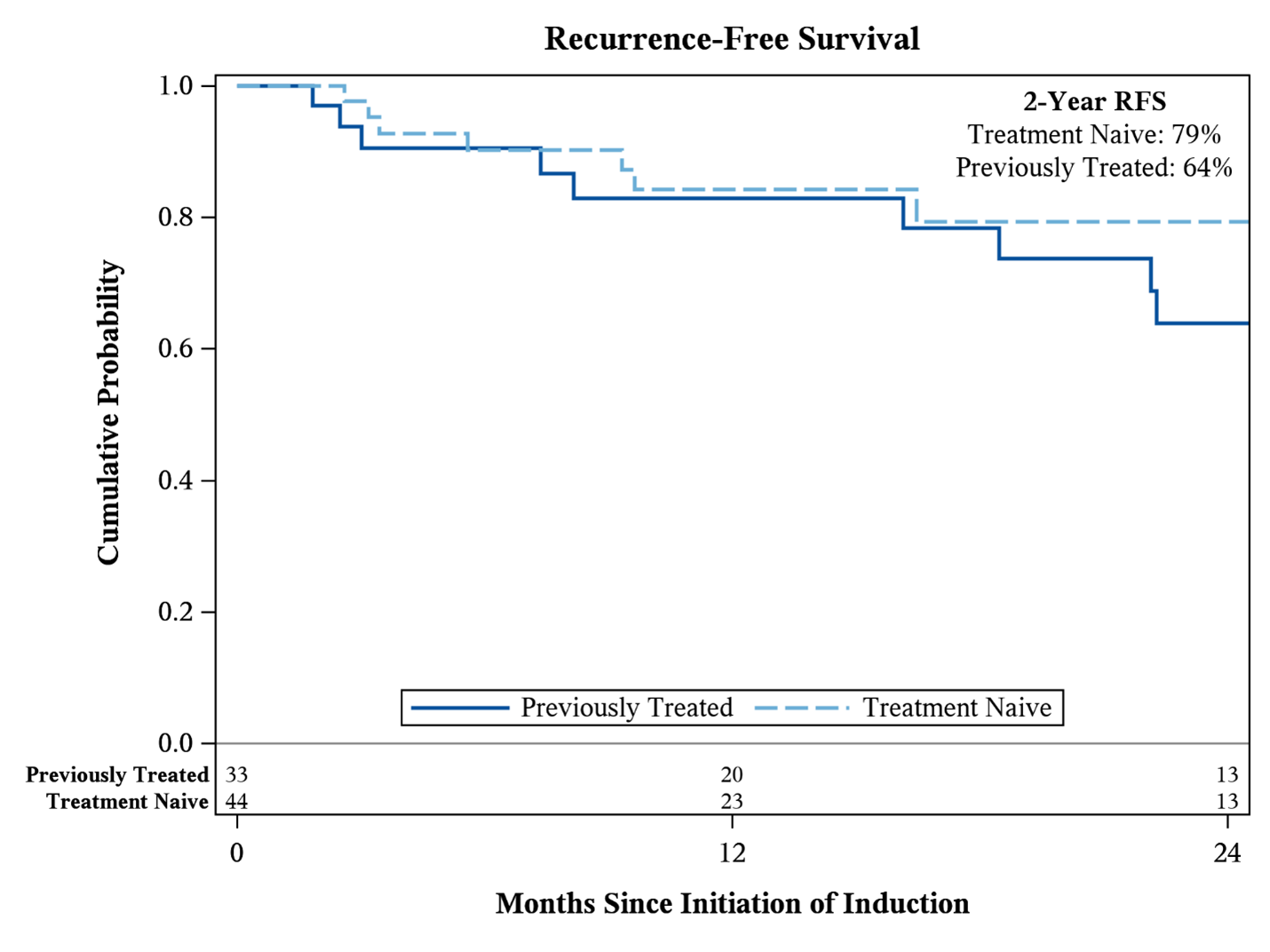
Introduction: Adjuvant intravesical therapy is recommended for patients with intermediate-risk NMIBC. While intravesical gemcitabine-docetaxel (Gem/Doce) has demonstrated favorable outcomes for high-risk NMIBC, its utility in the intermediate-risk setting is not well-described. We report efficacy and tolerance outcomes of Gem/Doce as an adjuvant treatment for intermediate-risk NMIBC. Methods: We retrospectively identified all patients with intermediate-risk NMIBC by AUA criteria who were treated with Gem/Doce between March 2012 and July 2022. Patients were treated with weekly sequential intravesical instillations of 1 g gemcitabine and 37.5 mg docetaxel for 6 weeks. Monthly maintenance of 2 years was initiated if disease free at first follow up. The primary outcome was recurrence-free survival (RFS). Survival was assessed using the Kaplan-Meier method, indexed from start of Gem/Doce induction. Surveillance was performed according to AUA guidelines. Results: The cohort included 77 patients with median follow-up of 26 (IQR: 14-50) months. Prior to Gem/Doce induction, 67 (87%) patients presented with TaLG, 3 (3.9%) with isolated <3cm TaHG, 5 (6.5%) with TaLG plus focal TaHG, and 2 (2.6%) with T1LG. A total of 33 (43%) patients received previous intravesical therapy with a median of 1 (IQR: 1-2) prior induction courses. There were 23, 13, and 13 patients with at least 1 previous induction course of BCG, single-agent docetaxel, and mitomycin, respectively. The 2-year RFS was 71% among all patients. Patients who were treatment naïve had superior RFS compared to those previously treated (p=0.04, Figure 1); 2-year estimates were 79% and 64%, respectively. There were 3 patients with a HG recurrence during the study period. There were 29 (38%) patients with adverse events; all were Grade 1-2 except one (1.3%) Grade 3 (acute oxygen desaturation). The most frequent adverse events were urinary urgency/frequency (10.4%), bladder spasms (9.1%), and UTI (5.2%). Three (3.9%) patients did not tolerate a full induction course. Conclusions: In a heterogenous population of patients with intermediate-risk NMIBC, Gem/Doce was an effective and well-tolerated adjuvant therapy. Further prospective evaluation is needed. SOURCE OF Funding: This work was supported by the John & Carol Walter Family Foundation and the Cancer Center Support Grant.