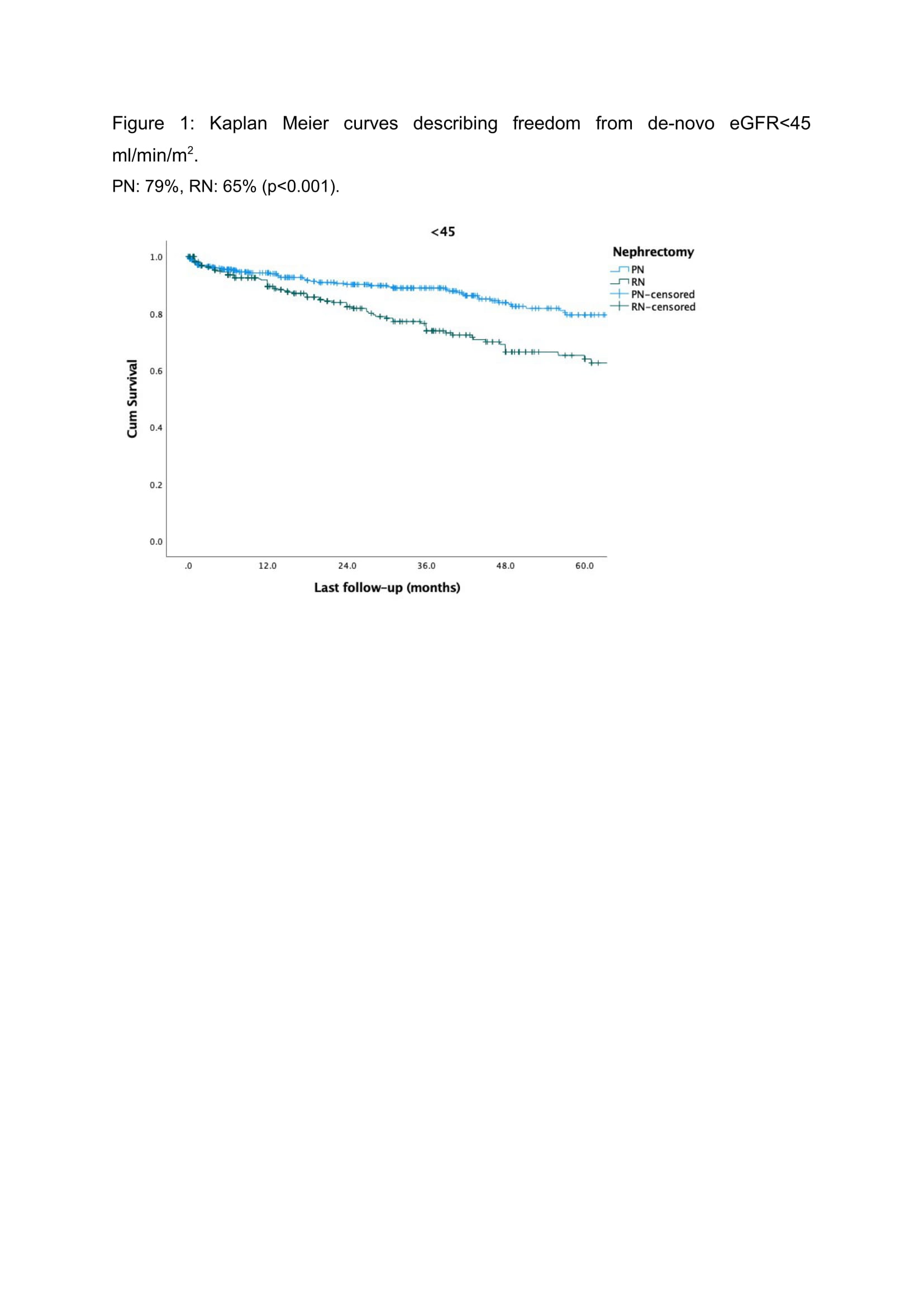
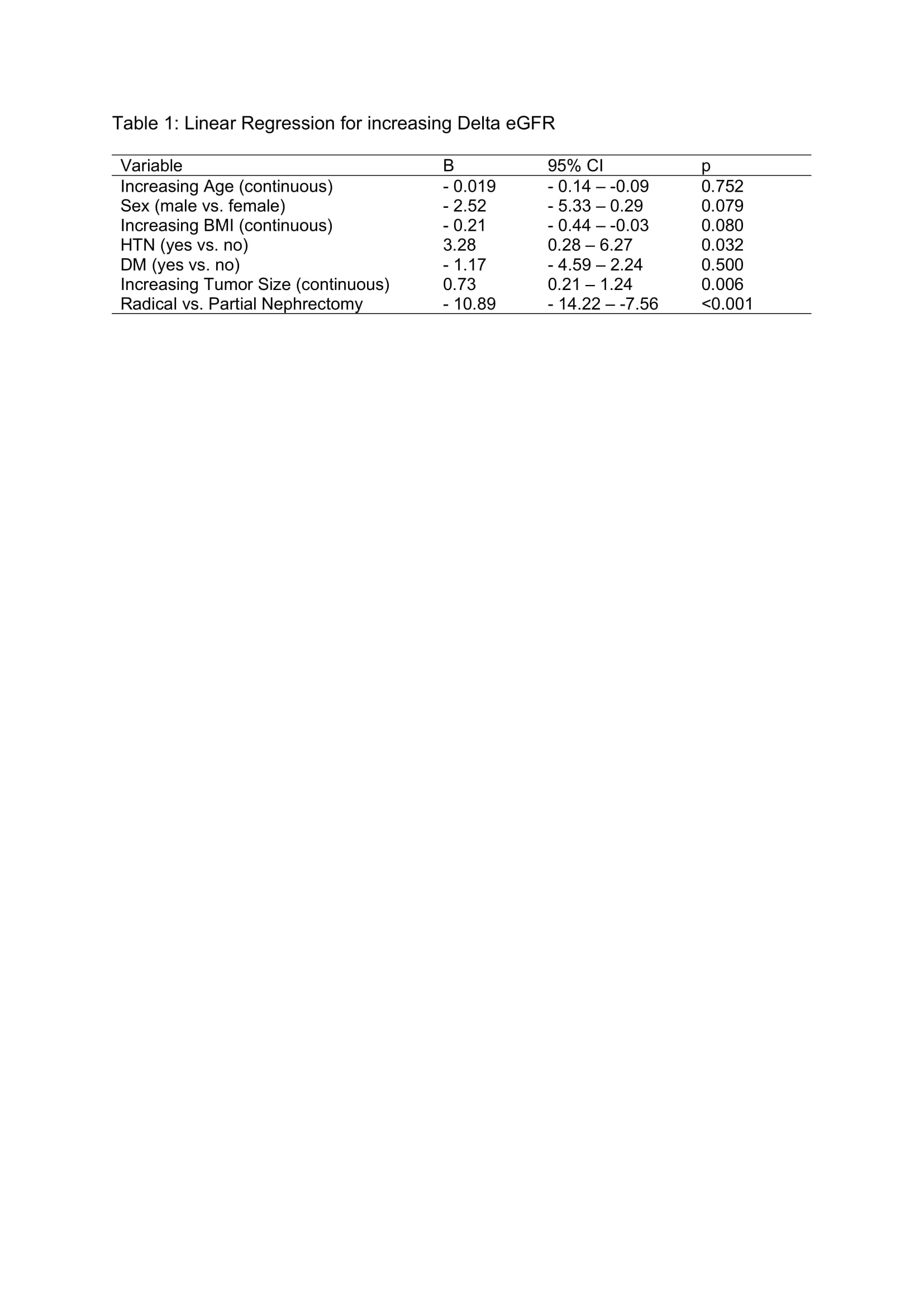
Introduction: Utility of Partial Nephrectomy (PN) for complex renal mass (CRM) is controversial. We determined the impact of surgical modality on post-operative renal functional outcomes for CRM. Methods: We retrospectively analyzed a multicenter registry (ROSULA). CRM was defined as RENAL score 10-12. The cohort was divided into PN and radical nephrectomy (RN) for analyses. Primary outcome was development of de-novo estimated glomerular filtration rate (eGFR) <45 ml/min/1.73m2. Secondary outcomes were de-novo eGFR <60 and DeGFR between diagnosis and last follow-up. Cox proportional hazards was used to elucidate predictors for de-novo eGFR <60 and <45. Linear regression was utilized to analyze DeGFR. Kaplan-Meier Analysis (KMA) was performed to analyze 5-year freedom from de-novo eGFR <60 and <45. Results: We analyzed 969 patients (RN=429, PN=540; median follow-up 24.0 months). RN patients had lower BMI (p < 0.001) and larger tumor size (p < 0.001). Overall post operative complication rate was higher for PN (p < 0.001), but there was no difference in major complications (Clavien III-IV; p=0.702). MVA demonstrated age (HR=1.05, p<0.001), tumor size (HR=1.05, p=0.046), RN (HR=2.57, p<0.001), and BMI (HR=1.04, p=0.001) to be associated with risk for de novo eGFR <60 ml/min/1.73m2. Age (HR=1.03, p<0.001), BMI (HR=1.06, p<0.001), baseline eGFR (HR0.99, p=0.002), tumor size (HR1.07, p=0.007) and RN (HR=2.39, p<0.001) were risk factors for de novo eGFR <45 ml/min/1.73m2. RN (B= -10.89, p<0.001) was associated with greater DeGFR (Table 1). KMA revealed worse 5-year freedom from de-novo eGFR <60 (71% vs. 33%, p<0.001) and de-novo eGFR <45 (79% vs. 65%, p<0.001) for RN (Figure 1). Conclusions: PN provides functional benefit in selected patients with CRM without significant increase in major complications compared to RN and should be considered when technically feasible. SOURCE OF Funding: None

 photo")