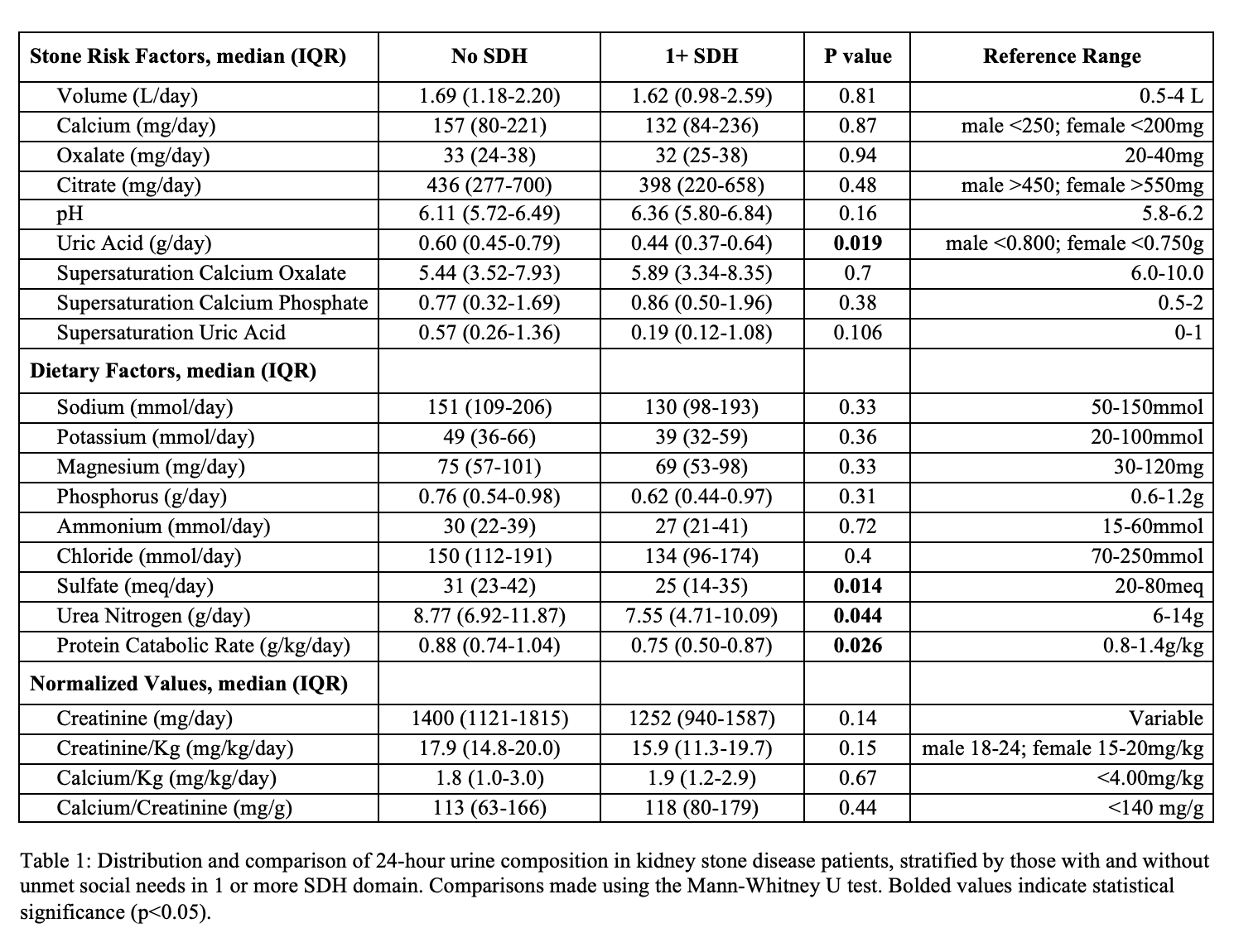
Introduction: Social determinants of health (SDH) are economic and environmental conditions that influence patients’ health. While dietary and environmental factors are known to influence kidney stone disease (KSD) risk, the effects of SDH have not been well explored. We used a validated 10-item social needs screener (SNS) to assess the relationship between SDH and 24-hour urine composition in patients with nephrolithiasis. Methods: Between 04/2018 and 06/2022, the SNS tool was implemented as a population health initiative in the primary care clinic of our institution, which acts as a safety-net hospital in a low-resource, urban setting. We retrospectively identified the patients who were referred to urology and underwent 24-hour urine collection for KSD evaluation. The SNS included questions on housing, utilities, finances, transportation, healthcare costs, and other SDH needs. Patient demographics, comorbidities, and 24-hour urine parameters were compared between those with and without self-reported unmet SDH needs. Results: Of the 5,403 patients referred to urology who previously completed the SNS, 1,456 had a diagnosis of nephrolithiasis and 124 completed a 24-hour urine analysis. Respondents were mostly female (64%) and Hispanic (56%). Consistent with the larger cohort of non-stone formers, 18 patients (15%) with recurrent nephrolithiasis expressed 1+ unmet SDH need. Those with SDH needs were more likely to be enrolled in Medicare/Medicaid than private insurance (94% vs 62%, p=0.007) and to have diabetes (72% vs 39%, p=0.008) when compared to those without social needs. On 24-hour urine analysis, those with 1+ SDH need had less urinary uric acid (0.44 vs 0.60, p=0.019), sulfate (25 vs 31, p=0.014), and urea nitrogen (7.55 vs 8.77, p=0.044), and a lower protein catabolic rate (0.75 vs 0.88; p=0.026). There were no differences in other 24-hour urinary parameters or stone composition. Conclusions: Patients with nephrolithiasis and unmet SDH needs have unique findings on 24-hour urinary testing. The use of a validated SDH screening tool may help to identify patients with KSD and unique risk factors for recurrence. Further prospective study is needed to explore this relationship and identify opportunities for improved nephrolithiasis treatment in patients with social and economic barriers to care. SOURCE OF Funding: None

 photo")