Resident Physician Columbia University Irving Medical Center
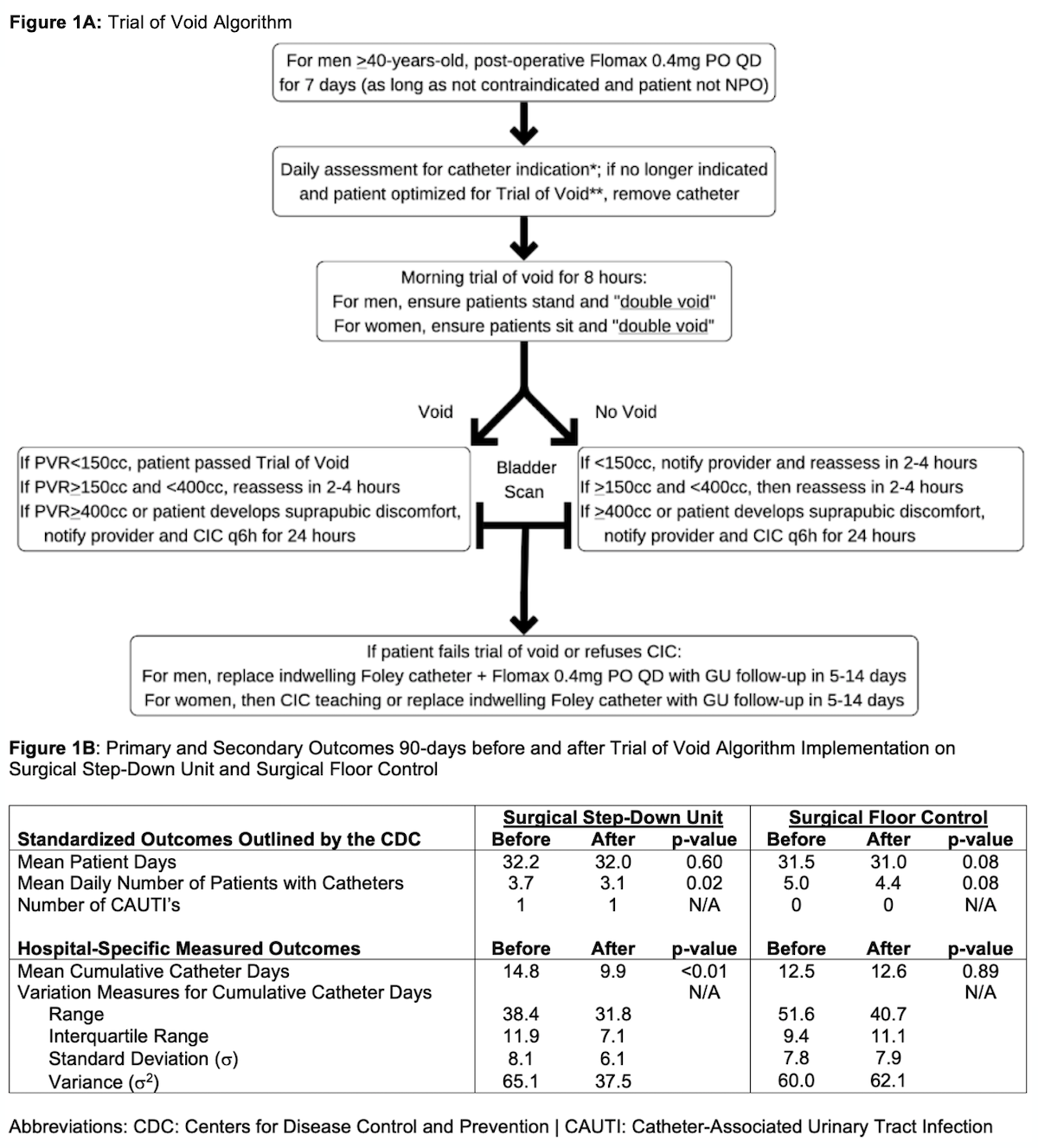
Introduction: Prolonged indwelling catheter use is a risk factor for catheter-associated urinary tract infections (CAUTIs). To reduce catheter use among post-operative patients, we sought to create and implement a novel algorithm to standardize the removal of indwelling Foley catheters. Methods: We partnered with nursing leadership and the General Surgery Department to develop an evidence-based trial of void algorithm for a surgical Step-Down Unit at an urban teaching hospital [Figure 1A]. Our cohort included post-operative patients treated with intraabdominal, thoracic, vascular, and gynecologic surgeries; patients having urologic surgeries with an imperative indication for a long-term indwelling urethral catheter were excluded from the algorithm but included in analysis. The primary outcome was mean cumulative indwelling urethral catheter days (ex. if 2 patients had catheters for 3 and 7 days, then cumulative catheter days would be 10). We also measured mean total patient days (as a surrogate for patient volume), mean daily number of patients with catheters, and the number of CAUTIs, which are all nationally reported outcomes from the Centers for Disease Control and Prevention. Another surgical unit where the algorithm was not implemented was used as a natural control. We analyzed changes in relevant outcomes 90 days before and after algorithm implementation. Results: The mean number of hospitalized patient days before and after algorithm introduction did not differ on the Step-Down Unit (32.2 vs. 32.0, p=0.60). After implementation, mean cumulative catheter days decreased (14.8 vs. 9.9, p<0.01), as did mean daily number of patients with catheters (3.7 vs. 3.1, p=0.02). Measures of catheter use variation also decreased [Figure 1B]. There was one CAUTI before and after algorithm implementation, the latter deemed potentially associated with algorithm non-adherence on root cause analysis. Measures of catheter use in the surgical floor control group did not differ for any outcome (p>0.05) over the same time-period. Conclusions: A multi-disciplinary approach to standardize catheter care with an evidence-based trial of void algorithm is feasible and effective in reducing catheter use. Further expansion of this pilot is needed to establish an impact on the associated rate of CAUTI. SOURCE OF Funding: None

 photo")