Session: PD39: Prostate Cancer: Detection & Screening V
PD39-04: mpMRI of the prostate in patients carrying a high clinical risk of prostate cancer diagnosis: is this imaging test necessary for diagnostic purposes in this subset of patients?
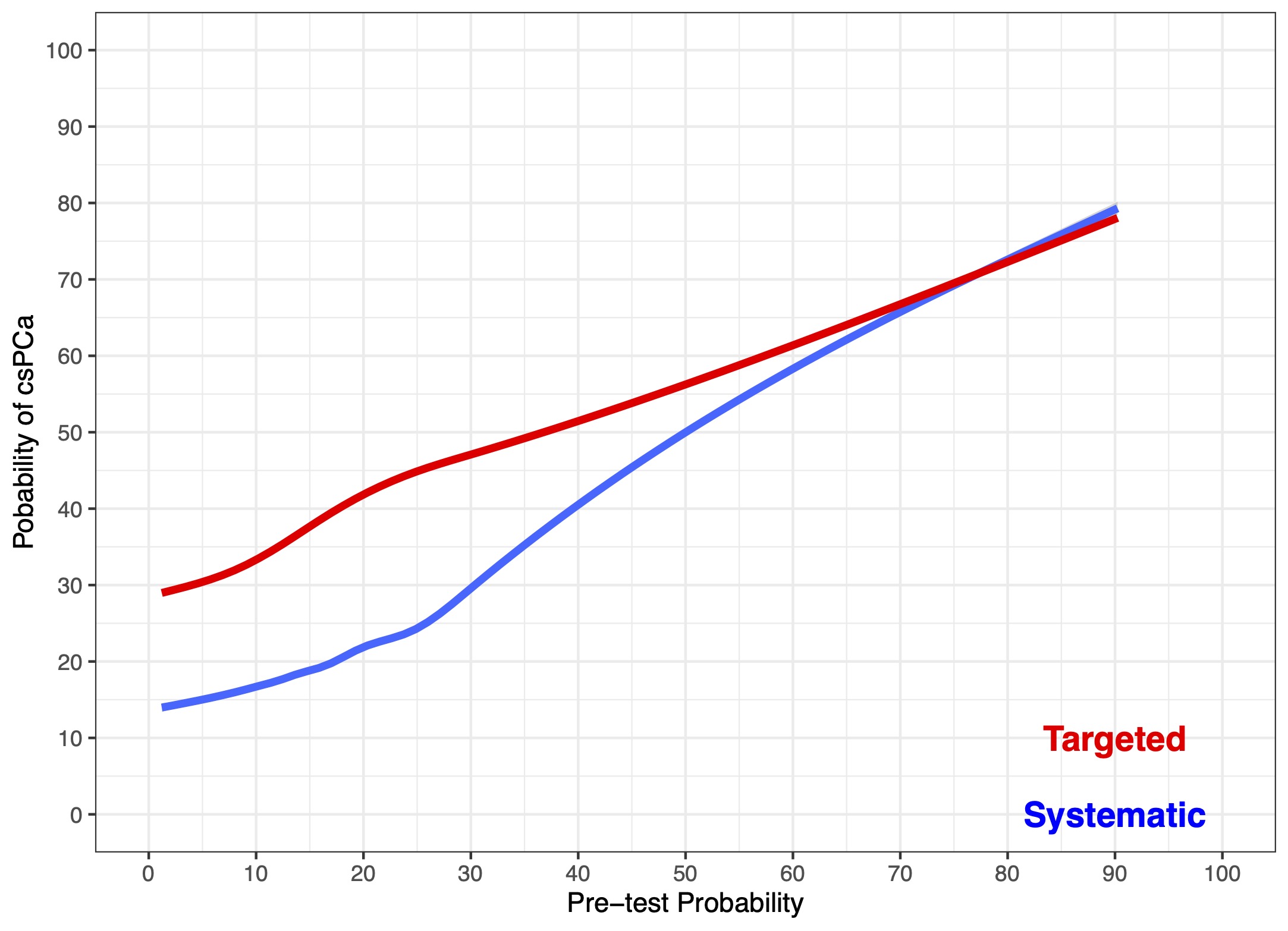
Introduction: mpMRI and subsequent targeted biopsy (TBx) significantly increases the detection of clinically significant prostate cancer (csPCa). However, its diagnostic benefit in men with a high clinical risk of PCa remains controversial. We hypothesised that not all patients with a clinical suspicion of PCa may benefit from mpMRI for diagnostic purposes. Specifically, the added value of TBx in patients with high risk of having CSPCa may be negligible. Methods: We identified 3,639 patients with clinical suspicion of PCa and suspicious mpMRI (PI-RADS=3) that received a SBx + TBx at 10 referral centres between 2014-2022. We then compared the detection of csPCa between SBx and TBx, according to the individual patient risk of having csPCa in order to assess the added benefit of TBx over SBx. We used a multivariable logistic regression analysis (MVA) to predict the risk of csPCa at prostate biopsy relying on clinical and radiological characteristics such as age, PSA, digital rectal examination, and PI-RADS. We then used loess non-parametric analysis to graphically explore the probability of csPCa at TBx vs SBx according to the pre-test probability of csPCa diagnosis calculated at MVA, hence comparing the diagnostic benefit related to each biopsy technique in terms of csPCa detection. Results: 1,491 (41%) patients had positive DRE and >86% had a PI-RADS 4-5 lesion at mpMRI. The median number of total and TBx cores taken was 14 and 4, respectively. csPCa incidence was 80%. Fig. 1 shows the variation of csPCa detection of TBx vs SBx according to individual risk of having csPCa. The detection of csPCa in TBx vs SBx ranged from 15% vs 30% (p < 0.001) to 80% vs 81% (p=0.3), for patients with very-low and very-high risk of having csPCa, respectively. The diagnostic benefit of adding TBx to SBx was highest in men with low risk of having csPCa (delta = 15%). Conversely, in men with a risk higher than 60%, csPCa detection in TBx vs SBx were similar. Conclusions: The added benefit of TBx to SBx in men with suspicion of PCa and concomitant positive mpMRI is highest in patients with low-intermediate risk of harboring csPCa. In patients with high clinical risk of having csPCa, adding TBx was not informative. The use of mpMRI in patients at high risk of csPCa is questionable for diagnostic purposes. SOURCE OF Funding: NA