Session: PD41: Benign Prostatic Hyperplasia: Surgical Therapy & New Technology V
PD41-11: The Impact of Prostate Volumes (≤80 cc vs. > 80 cc) on Perioperative Outcomes and Risk of Retreatment in Patients Undergoing Aquablation: A Single-Center Study
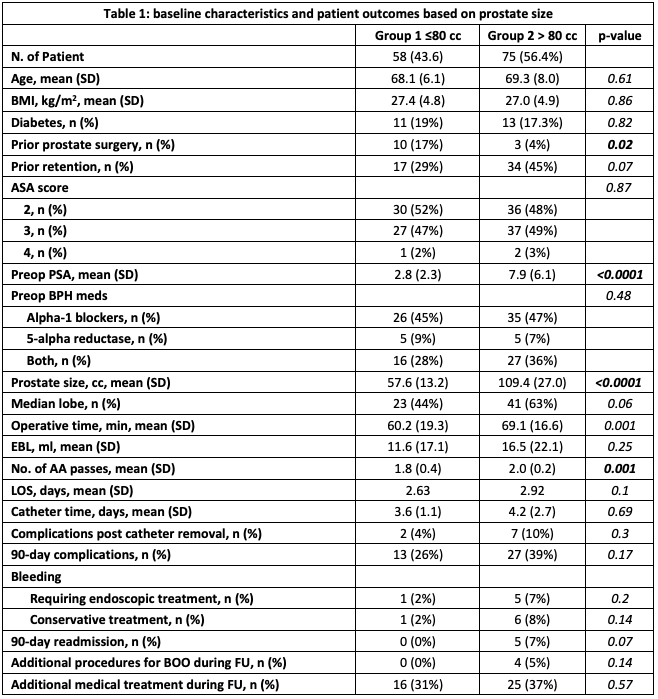
Introduction: Aquablation (AA) therapy is a promising alternative for the treatment of lower urinary tract symptoms secondary to an enlarged prostate. Though generally shown to be safe in patients with larger prostates and novel image-guiding software simplifies treatment, prostate volume (PV) could have implications on the perioperative course. The goal of this study was to determine if PV has an impact on perioperative outcomes following AA therapy. Methods: 133 patients underwent AA therapy at our institution between 2020-2022. Patients were stratified based on small (=80cc) and large (>80cc) PVs. Patient data on baseline characteristics and peri- and postoperative outcomes were retrospectively collected. Outcomes of interest included 90-day complication rate, bleeding requiring retreatment, and 90-day readmission rate and retreatment for bladder outlet obstruction (BOO) within the follow-up (sig. p <0.05). Results: A total of 58 (44%) have a PV = 80 cc (group 1), while 75 (56%) of patients have a PV >80 cc (group 2). In group 1, the PV was 57.6ccs while in group 2 the mean was 109.4ccs. There was no difference in age (68.1 v 69.3, p=0.61), BMI (27.4 v 27, p=0.86), and ASA score (ASA 3, 47% v 49%, p=0.87). A small prostate was associated with any prior prostate surgery, including prior resection (17% v 4%, p=0.02) and a large prostate was associated with prior retention (29% v 45%, p=0.07) and likelihood of having an identifiable median lobe (44% v 63%, p=0.06). A higher number of AA passes (1.8 v 2.0, p=0.001) and operative time (60.2 v 69.1 min., p=0.001) were associated with a large prostate, while there was no difference in EBL (11.6 v 16.5 ml, p=0.25). There was no statistically significant difference in 90-day complications (26% v 39%, p=0.17), postoperative bleeding requiring endoscopic treatment (2% v 7%, p=0.2), and 90-day readmission (0% v 7%, p=0.07) based on prostate size. The risk of retreatment of BOO during the follow-up was comparable between the 2 cohorts (0% v 5%, p=0.14). Conclusions: Overall, patients undergoing AA therapy experienced low rates of perioperative complications, bleeding, or retreatment and are independent of baseline PV. This provides an attractive transurethral minimally invasive alternative to patients with larger prostate glands and LUTS. SOURCE OF Funding: NA