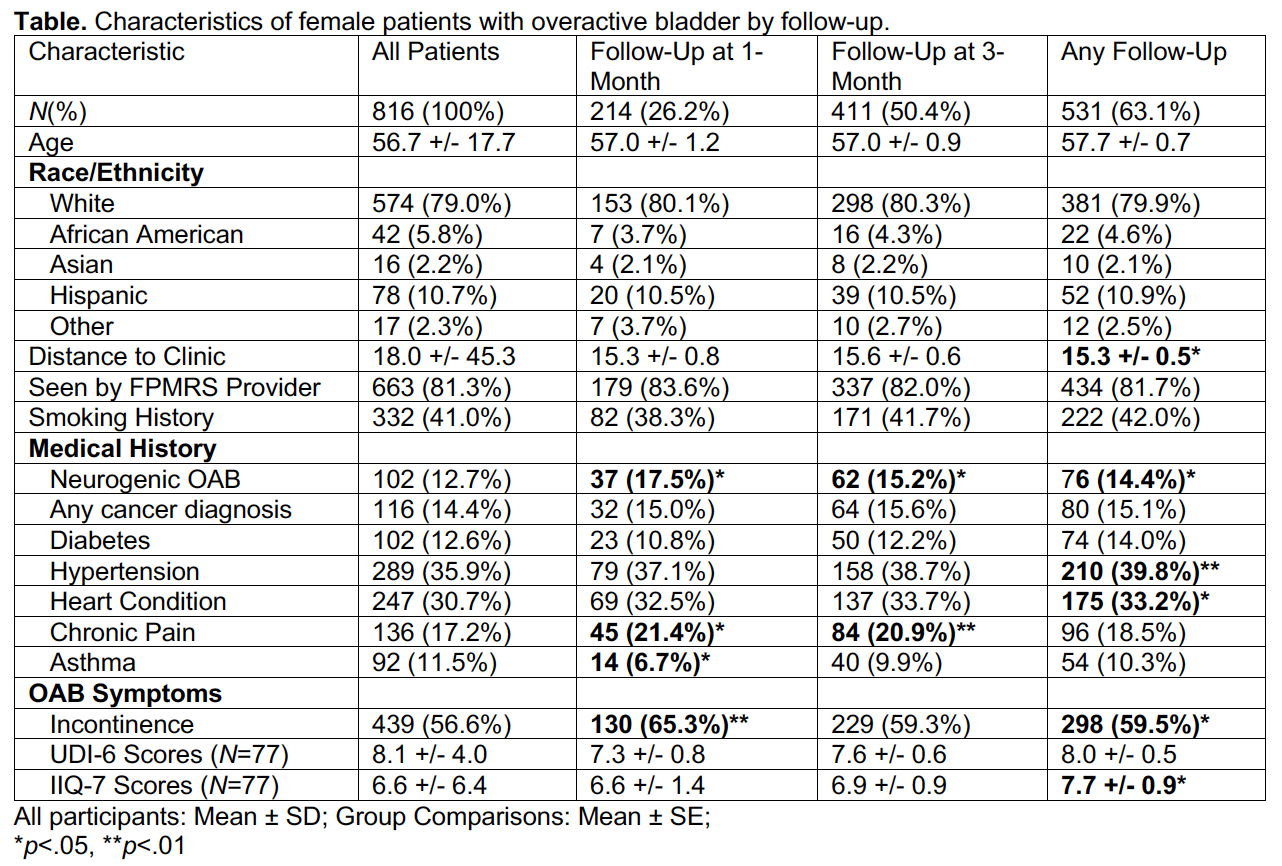
Introduction: Overactive bladder (OAB) is a common condition responsible for significant morbidity in female patients. Treatment can be complex and multifaceted, requiring strict treatment compliance and often several clinical encounters for effective symptom management. Recognizing risk factors for loss to follow-up is critical to identifying patients who may require supplementary interventions to improve adherence. Methods: Adult female patients presenting for a new patient visit for OAB symptoms (frequency, urgency, incontinence, nocturia) were identified at an outpatient urology clinic between July 2020 and June 2021. Medical records were abstracted for demographic data, smoking history, medical comorbidities, and baseline OAB symptom severity. Prospective chart review was performed to identify additional urology clinic visits for any reason at 1-month, 3-month, and present-day time horizons. The Student’s t-test for quantitative variables and the chi-squared test for qualitative variables were used to compared characteristics of patients who did and did not have follow-up visits by those time horizons. Results: 816 female patients were included in the analysis, of which 63.1% had a follow-up visit recorded between the initial visit and present-day. There was no difference in follow-up by age or race (see Table). Patients with follow-up visits within the catchment period were more likely to live closer (p <.05), have neurogenic OAB (p <.05), and endorse incontinence (p <.05). They were also more likely to have a history of hypertension (p <.01) and heart disease (p <.05), and at the 1-month and 3-month time horizons to report a history of chronic pain (p <.05 and p<.01, respectively). Conclusions: This study recapitulates known associations between distance to clinic and baseline symptom severity with chance of follow-up, but also reveals a correlation between follow-up for overactive bladder and certain medical comorbidities, which may provide real-world evidence for the potential role of multidisciplinary approaches in the treatment of OAB. The lack of age-based and racial inequity in follow-up rates is also noteworthy. Further research could target interventions to reduce attrition through the creation of a hazard score to identify patients at high-risk for loss to follow-up. SOURCE OF Funding: None.