Session: MP76: Benign Prostatic Hyperplasia: Surgical Therapy & New Technology IV
MP76-09: Schelin CatheterTM for Trans Urethral Intraprostatic Anesthesia before Rezūm Water Vapor Treatment: a new tool to enhance the minimal invasiveness
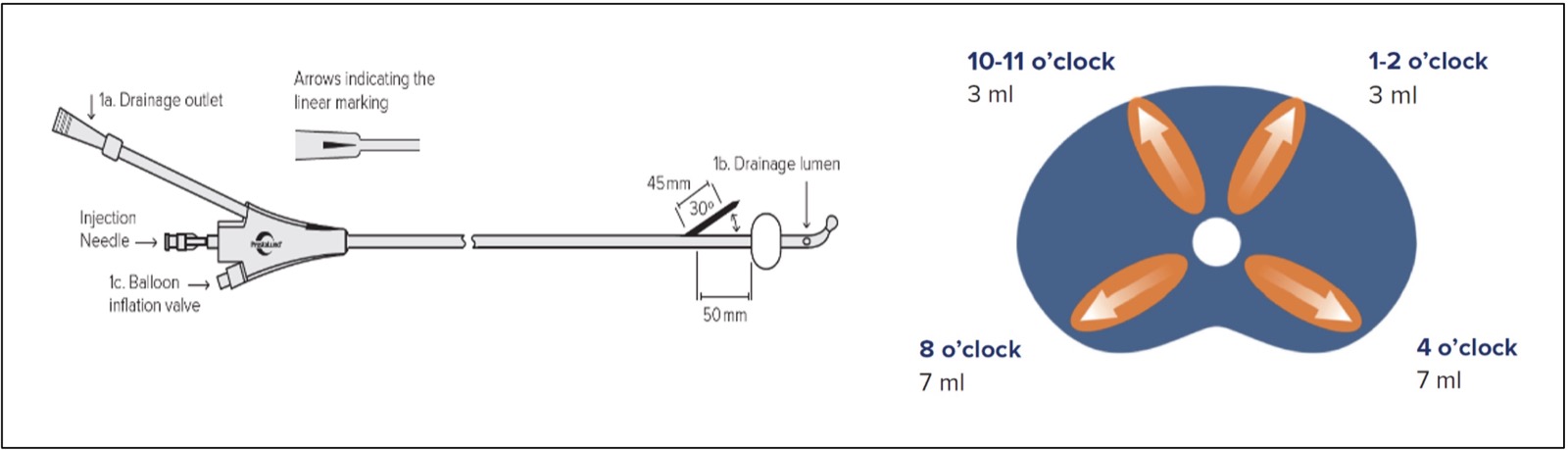
Introduction: Among minimally invasive surgical techniques (MISTs) for moderate lower urinary tract symptoms (LUTS) due to benign prostatic obstruction (BPO), Rezu¯mTM water vapor treatment (Boston Scientific Corporation, Marlborough, USA) (RT) has been accepted as one of the most effective and versatile, with a very good sexual safety profile. To further enhance the minimal invasiveness of RT, we sought to evaluate potential advantages and feasibility of pure local transurethral intraprostatic anesthesia (TUIA) via the Schelin CatheterTM (ProstaLund AB, Lund, Sweden) (SC), a 3 ways device designed with an operational channel equipped with a retractile needle and the standard drainage and ballon ports (Figure 1). Methods: After Ethical Commitee approval, included and collected data from 20 patients with moderate LUTS due to BPO, undergone RT procedure using TUIA by SC, from 2 centers. To rate their pain, patients were asked to use a numeric rating scale (NSR; numbered 0–10; 0 “No pain”/10 “Worst pain”) at 9-time points: 1-Preoperatively; 2-Schelin catheter insertion; 3-anestethic infiltration; 4-Rezum probe insertion; 5-Water Vapor Treatment (WVT); 6-Catheter insertion; 7-Day 1; 8-Day 7 catheter removal; 9-Day 30 follow-up visit. Results: All 20 patients safely received TUIA prior RT. None required further anesthesiologic treatment. Median prostate size, Qmax, IPSS and QoL were 75ml, 9 mL/sec, 23 and 4, respectively. Median TUIA time was 3 minutes. Median catheterization time was 7 days. No need of re-catheterization or urinary tract infections at 30 days post-operatively were reported. Median NRS reported was 1.5 at each time point except at point 1, 2, 3 and 5. At preoperative stage NRS of pain was 0 in all cases. During catheter insertion (point 2) median NRS of pain was 2; during LA infiltration (point 3) was 2.5, and during WVT was 2 (point 5). One out of 10 patients reported a NRS of 6 during WVT (point 5). No perioperative anesthesiologic and procedure-related complications were recorded. Conclusions: Our data report for the first time in literature the feasibility and safeness of TUIA during RT using SC that showed full operative and post-operative pain control and reduced operative time and patient discomfort. SOURCE OF Funding: none