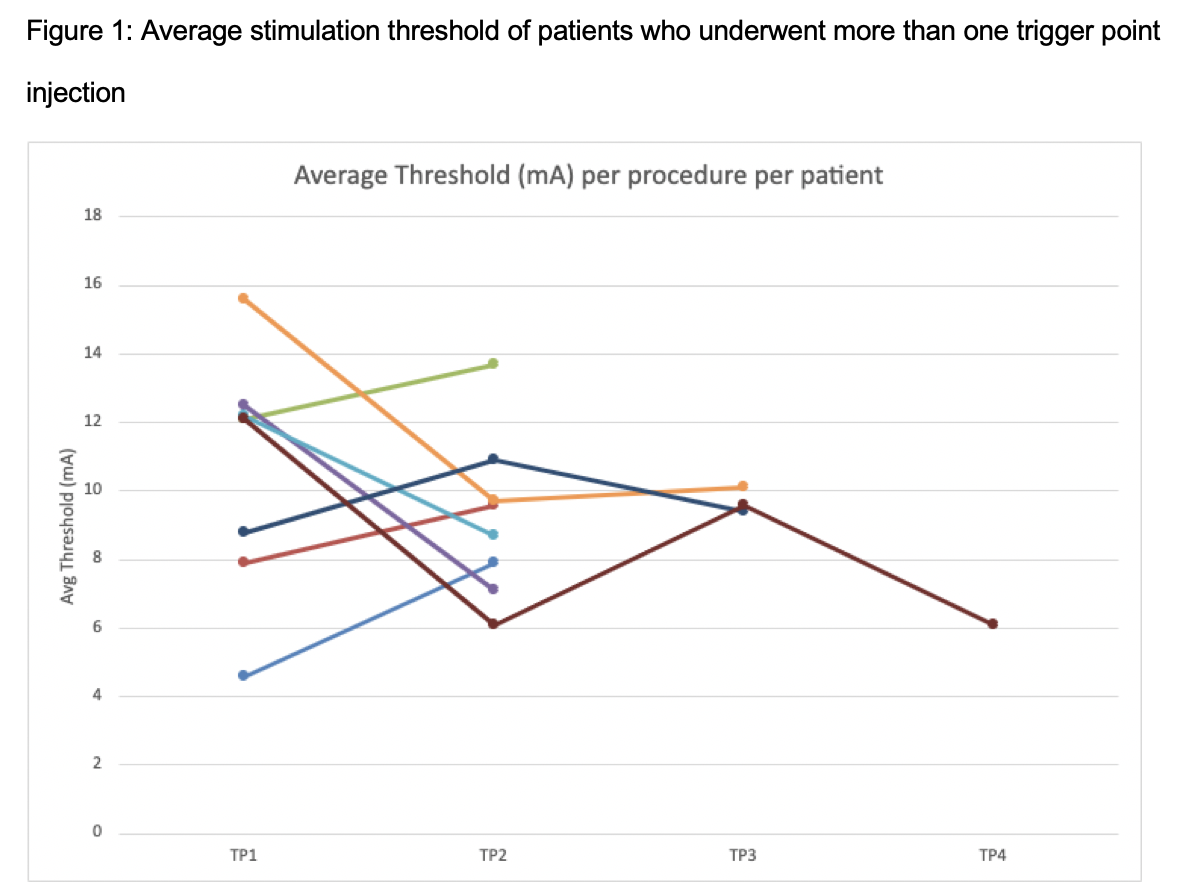
Introduction: Pelvic floor trigger point injections (PFTPI) are an established therapy in the management of patients with myofascial pain. Commonly, botulinum toxin (BTA) is injected into the pelvic floor using digital palpation of the muscles. This is an imprecise method of delivery, as there is no objective confirmation of drug delivery to the desired location. We propose a technique using a peripheral nerve stimulator (PNS) to precisely isolate the muscles during PFTPI. Methods: We conducted a retrospective review of patients with myofascial pain who had PFTPI using a PNS (LifeTech NS-2CA DualStim Plus) between 9/1/2020-8/31/2022. 50-100u of BTA reconstituted with 20 mL saline was injected into the levator ani complex at 1, 3, 5, 7, 9, and 11 o'clock. A insulated needle was inserted into the muscle while connected to the PNS. Placement was confirmed when the muscle twitch was palpated. Motor response thresholds were obtained by reducing the PNS amplitude until the muscle twitch was no longer appreciated. We aim to describe the procedure and intraoperative characteristics of patients receiving TPI with PNS. Our secondary objective is to compare patients who did and did not receive subsequent injections. Results: A total of 15 patients underwent 27 injections. 8/15 (53%) received >1 injection. The mean age was 48 yr and 3 patients were male. 67% were non-Hispanic white. This procedure was always combined with another intraoperative procedure (cystoscopy n=3, intradetrusor BTA n=18, urethral sphincter or bladder neck BTA n=6). Mean operative time was 48 minutes (range 29-106). The average interval between injections was 163 days (range 98-364). In comparing those who did or did not undergo a repeat injection procedure, there was no difference in age (48 vs 47 years, p=0.95), BTA units (93.8 vs 71.4, p=0.30), concomitant procedure type, or the average threshold of injection sites (10.7 mA vs 9.8 mA, p=0.57). Among patients who had more than one injection, there was no relationship between average threshold over time (Figure 1). Conclusions: In this pilot study we demonstrate that pelvic floor TPI with PNS is reliable and reproduceable. Though we lack standardized assessment of benefit, over 50% of patients returned for repeat injections. Further study is needed to compare outcomes of TPI with and without this technique. SOURCE OF Funding: None