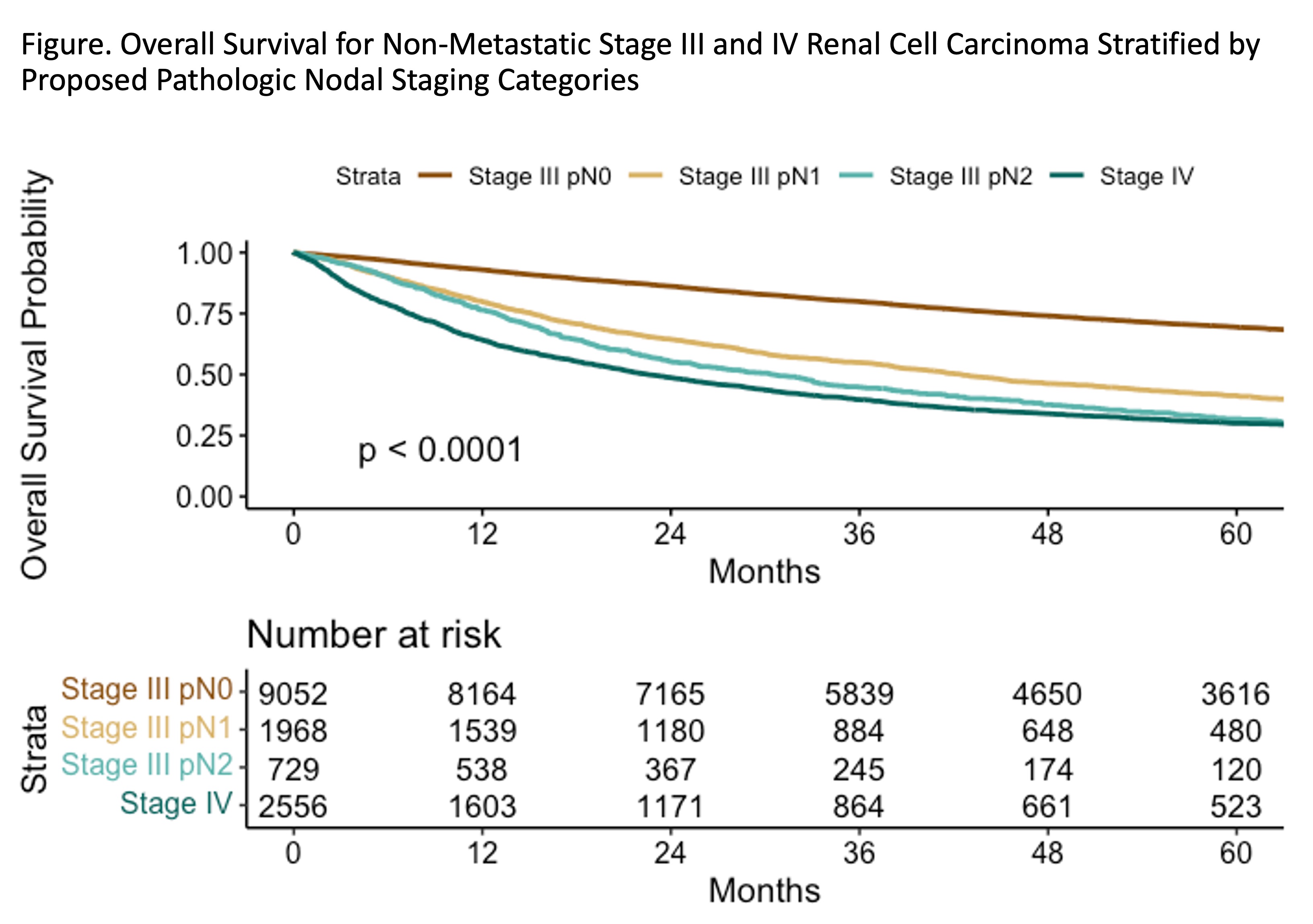
Introduction: The prognostic significance of lymph node (LN) positivity in renal cell carcinoma (RCC) is poorly understood. Currently, American Joint Committee on Cancer (AJCC) Stage III RCC includes both node-positive pN1 and node-negative pN0 disease. We hypothesize that (1) there is a threshold in number of pathologic positive LN (pLN) that distinguishes favorable from poor risk nodal disease, and (2) current categorization of pN1 can be subdivided into pN1 and pN2 based this threshold. We tested our hypothesis using the National Cancer Database (NCDB). Methods: From 2004-2019, all RCC were queried in patients age =18. pN1 RCC with no synchronous metastasis were selected to minimize confounding from metastatic burden. Multivariable Cox regression tested association between number of pLN and all-cause mortality (ACM). Receiver Operator Characteristic (ROC) Curve analyses employing concordance probability method and analysis of regression coefficients evaluated performance of potential cut-points for pN2. Kaplan-Meier analyses (KMA) compared these thresholds against overall survival (OS) in non-metastatic Stage IV RCC. Results: 29,388 patients were identified; 3910 (13.3%) had pN1. On Cox regression, increased number of pLN was associated with increased hazard of ACM (HR 1.19, p<0.001). Analysis of estimated regression coefficients identified potential threshold at =3 pLN. ROC mapping of thresholds =2 to =10 showed stable concordance probability 0.26-0.33, AUC=0.656. On KMA, when threshold was =3, 5-year OS was no longer significantly different from non- metastatic Stage IV RCC as illustrated by overlapping confidence intervals. We designated pN1 as 1-2 pLN, and pN2 as =3 pLN. 5-year OS for Stage III pN0 was 69.4% (95% CI 68.4-70.5), for Stage III pN1 was 41.4% (39.0-43.8), for Stage III pN2 was 31.8% (28.2-35.9%), and for non-metastatic Stage IV was 30.0% (28.2-32.0%). pN2 exhibited 38% greater hazard of ACM (HR 3.31, p<0.001) compared to pN1 (HR 2.39, p<0.001). Conclusions: These findings show that original pN1 RCC could be stratified to pN1 and pN2, with pN2 conferring poor prognosis comparable to non-metastatic Stage IV pN0 disease. Although validation studies are warranted, consideration should be given towards stratifying Stage III pN2 patients to a higher risk group. SOURCE OF Funding: None