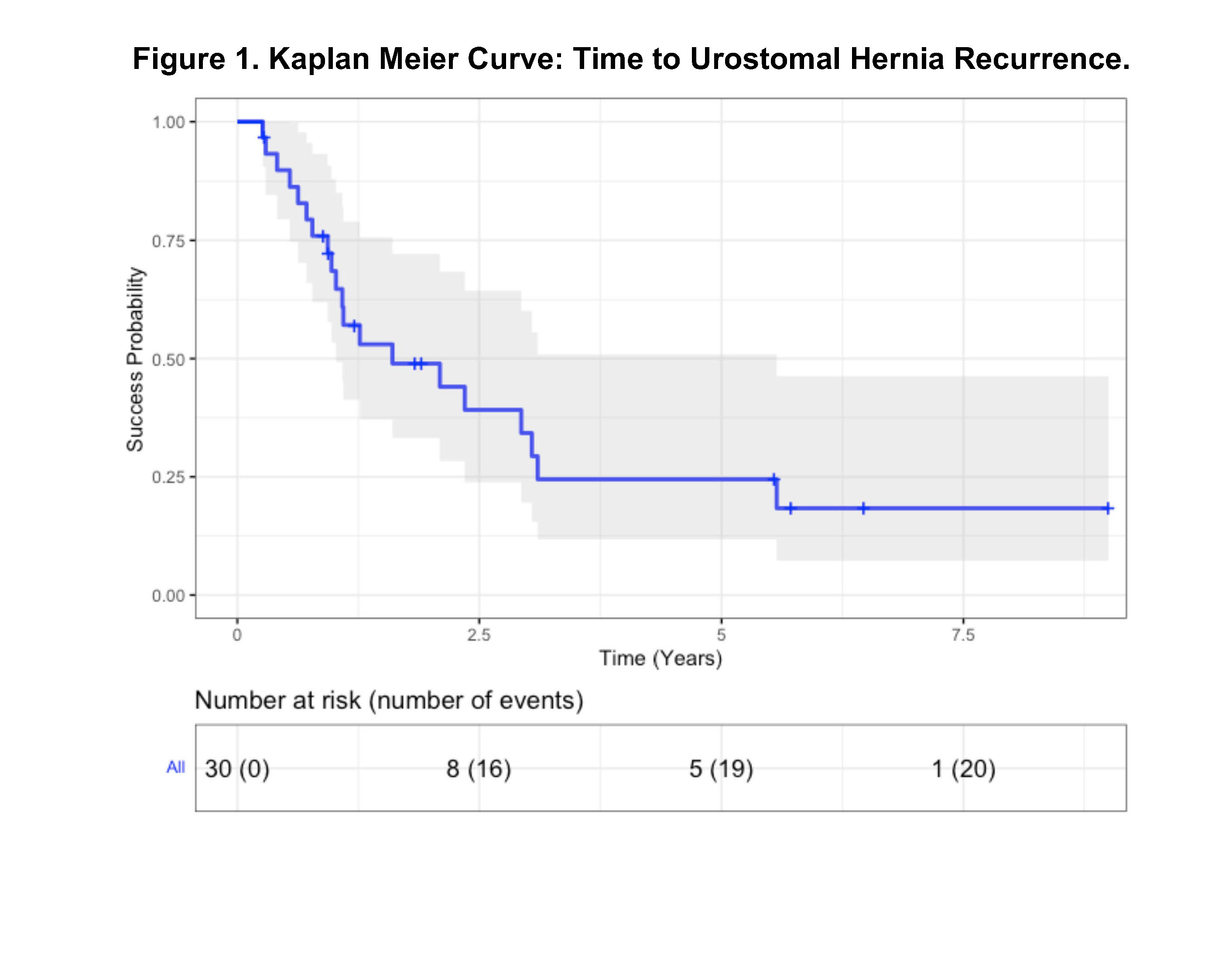
Introduction: Following urinary diversion, a challenging complication is parastomal hernia formation, termed here as urostomal hernia. We examine patients who underwent urostomal hernia repair and describe their outcomes. Methods: For individuals who underwent urostomal hernia repair, we collected retrospective demographic data, perioperative variables, surgical technique, and tracked hernia recurrence events. Kaplan Meier methods were used to estimate time from hernia repair to hernia recurrence. Cox proportional hazards modeling assessed risk factors for hernia recurrence. Results: Thirty patients had a urostomal hernia repair between 2009 and 2022. Urinary diversion was initially performed for benign (37%) or malignant (63%) pathologies. Median age was 68.5 [IQR: 57.5,73.8], 57% male, and a median Charleston comorbidity index of 8 [IQR: 6,10]. Primary indications for urostomal hernia repair were bowel obstruction or incarceration (n=10, 33%), obstructive uropathy (n=6, 20%), pain (n=5, 16%), pouching difficulty (n=5, 16%), and recurrent urinary tract infections (n=4, 13%). Follow up period was a median of 2.5 [IQR: 1,5] years. Repair techniques included primary repair (n=15, 50%), stomal relocation without mesh (n=5, 17%), mesh placement without stomal relocation (n=7, 23%), and mesh with stomal relocation (n=3, 10%). Nearly a third (30%) had a concurrent procedure at the time of hernia repair (eg, nephrectomy, ureteral reimplant, ventral hernia, new ileal loop). Urostomal hernia recurrence rate was 67%, occurring at a median of 13 [IQR: 8,26] months from initial repair. Kaplan Meier analysis of time to urostomal hernia recurrence is depicted in Figure 1. Twelve (40%) individuals had a second urostomal hernia repair and three (10%) had a third repair. No associations found within the Cox proportional hazards model which was limited by sample size. At last follow up, the primary urostomal hernia complications that prompted hernia repair had resolved in 22 individuals (73%). Conclusions: Recurrence following urostomal hernia repair is common (67%) even in the hands of experienced urology and general surgery teams. For these complex patients, perhaps a more important metric of success is resolution of primary hernia complications following repair, which is 73% in this cohort. SOURCE OF Funding: None