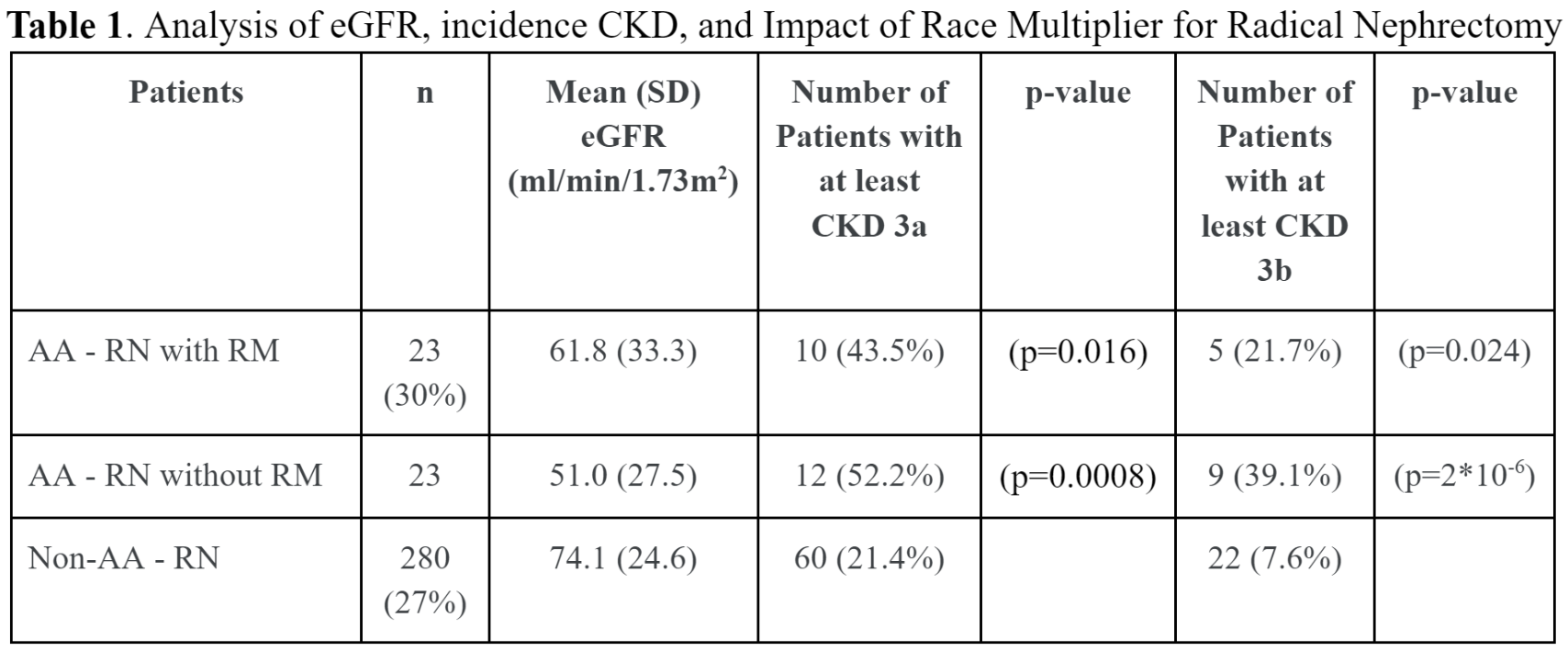
Introduction: In estimated glomerular filtration rate equations (eGFR), the race multiplier (RM) yields greater eGFR values and may assign less severe CKD stages to African-Americans (AA). When deciding on appropriateness for partial nephrectomy (PN) patients with CKD are often considered a relative or absolute indication for PN. We hypothesize that the eGFR RM may have potential ramifications for patients being counseled for radical (RN) vs. PN to manage their renal tumor. Methods: We utilized prospective and retrospective, IRB-approved single-center databases to select AA patients who underwent PN or RN between 2016 and 2022. Demographics, preoperative risk factors, preoperative eGFR with and without the RM and surgical management were collected. Descriptive statistics and two-tailed difference of proportion tests were used to compare the percentage of patients with CKD who underwent RN. Results: Out of 1139 patients who underwent RN or PN, 75 (6.6%) patients were AA. The RM vs. no RM mean ± SD preoperative eGFR was 76.3±26.1 vs. 62.9±21.5; incidence of CKD 3a were 22.7% vs. 38.7% (p=0.034); incidence of CKD 3b were 8.0% vs. 16.0% (p= 0.13), respectively. Table 1 summarizes the eGFR and incidence of CKD in AA with and without the RM compared to non-AA undergoing radical nephrectomy. We noted in all AA patients, regardless of using the RM, that the incidence of CKD3a and CKD 3b was significantly higher compared to non-AA undergoing RN. This difference was accentuated when removing the RM. Conclusions: We noted a statistically higher incidence of CKD in AA patients undergoing RN compared with non-AA patients. This difference was accentuated when removing the RM. Limitations include selection bias and small cohort of AA. These findings have potential ramifications for surgical planning of PN vs RN based on presence of CKD and may contribute to healthcare inequalities. SOURCE OF Funding: None