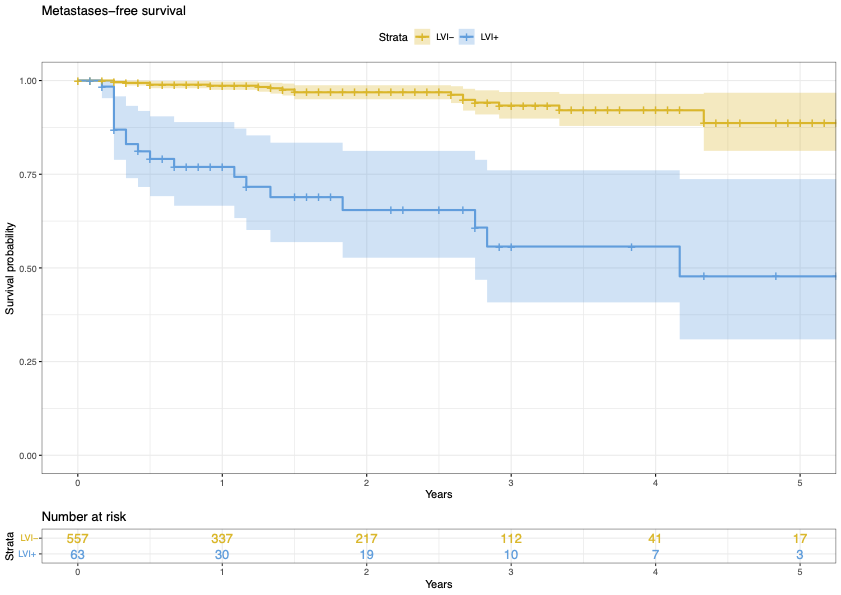
Introduction: Lymphovascular invasion (LVI) has been shown to be associated with higher grade and stage of prostate cancer. However, the literature is scarce on its ability to predict long-term oncological outcomes. Therefore, we aim to evaluate the impact of LVI on long-term prostate cancer outcomes following radical prostatectomy. Methods: A consecutive sample of patients with localised prostate cancer undergoing radical prostatectomy in a multicentre database was included in the analysis. Postoperative PSA measurements and clinical examinations were taken at 3, 6 and 12 months and afterwards yearly. Further diagnostic imaging was obtained with a rising PSA or clinical suspicion. Recurrence-free survival (RFS) and metastases-free survival (MFS) were analysed as a time-to-event outcome using Kaplan-Meier analyses with log-rank tests. To assess the effect of LVI, we created multivariable Cox proportional hazards models adjusting for relevant clinical and demographic characteristics. Ethics committee approval was obtained. Results: A total of 3,732 men were included for analysis with a median follow-up of 44 months. LVI was detected in 18% (n=682). LVI was more common with increasing ISUP grade [RR 4.2, 95%CI 3.8-4.6] and pathological stage [RR 6.5, 95%CI 5.9-7.2]. The incidence of metastasis at 5-years was 12%. Men that were LVI+ were more likely to develop metastatic disease than those that were LVI- (39% vs 6%, p<0.01). LVI was an independent predictor of metastasis [HR 2.2, 95%CI 1.7-3.0] and biochemical recurrence [HR 2.1, 95%CI 1.8-2.5]. This finding was consistently noted on subgroup analysis of men with both intermediate- and high-risk prostate cancer. Conclusions: Lymphovascular invasion is a prognostic indicator of adverse recurrence- and metastasis-free survival following surgery for prostate cancer. This can assist with risk-stratification following radical treatment and possibly aid decision-making regarding adjuvant treatment. SOURCE OF Funding: None