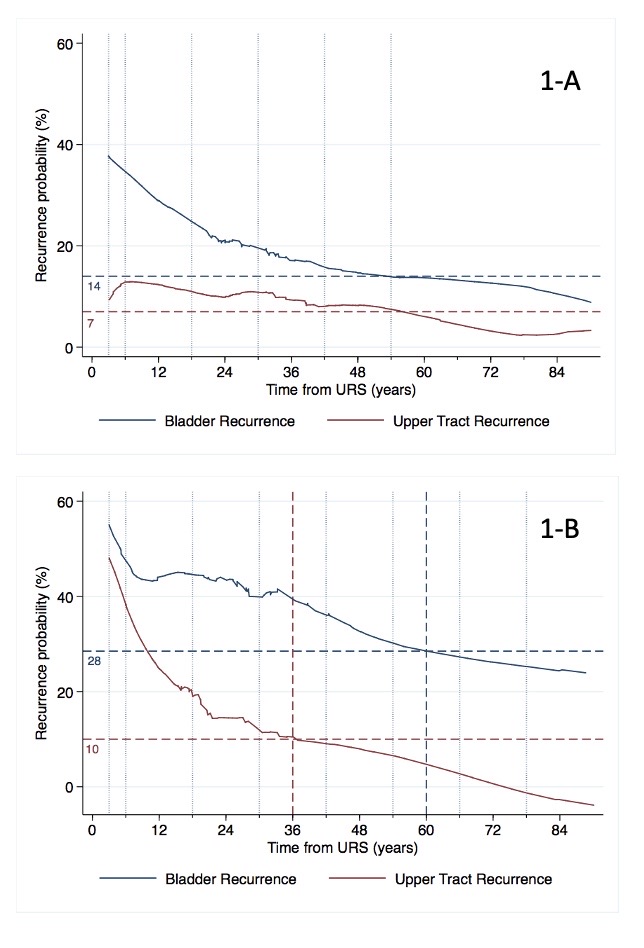
Introduction: The EAU guidelines on upper tract urothelial carcinoma (UTUC) have been implemented to provide separate recommendations on oncologic surveillance for low- and high-risk UTUC after nephron-sparing surgery (NSS). This study aimed to evaluate whether the surveillance scheme is accurate for patients with UTUC after NSS. Methods: We relied on a prospectively maintained database of patients who underwent NSS for UTUC between 2015-2021. Patients were followed up in compliance with the EAU guidelines. The crude risk of recurrence was evaluated against time from URS, with the Locally Weighted Scatterplot Smoothing. The risk of recurrence at the time points when imaging should be de-intensified according to the EAU guidelines was estimated. Results: Overall, 63 (39.4%) and 97 (60.6%) patients resulted in low- and high-risk groups as defined by the Guidelines, respectively. In the low vs high-risk group, 19% and 28.9% of patients had bladder recurrence during the follow-up. Conversely, 14.3% and 16.5% of patients had UTUC recurrence in the two cohorts. Figure 1 displays the risk of bladder and UTUC recurrence over time for the low- (1A) and high-risk group (1B), respectively. Vertical lines correspond to the time points when imaging should be obtained. For low-risk patients, bladder cancer recurrence is higher than 20% up to 24-months. At 60-month, timepoint after which imaging should be interrupted, the risk of bladder cancer recurrence was 14%, while the risk of UTUC recurrence was 7%. Conversely, for high-risk patients, the risk of bladder and UTUC recurrence at 36-months was approximately 40% and 10%, respectively. Conversely, at 60-month, the risk of bladder recurrence and UTUC recurrence was 28% and 8%, respectively. Conclusions: Our findings suggest that the surveillance scheme for patients with UTUC treated with NSS can be further improved. For low-risk patients, cystoscopy should be performed semi-annually until 24-months after RNU, while imaging should be obtained up to 60 months, as per current guidelines. For high-risk patients, imaging should be intensified to semi-annually up to 36-month after surgery, then obtained yearly thereafter; cystoscopy should be ideally performed semi-annually until 60-month, then yearly thereafter. SOURCE OF Funding: No