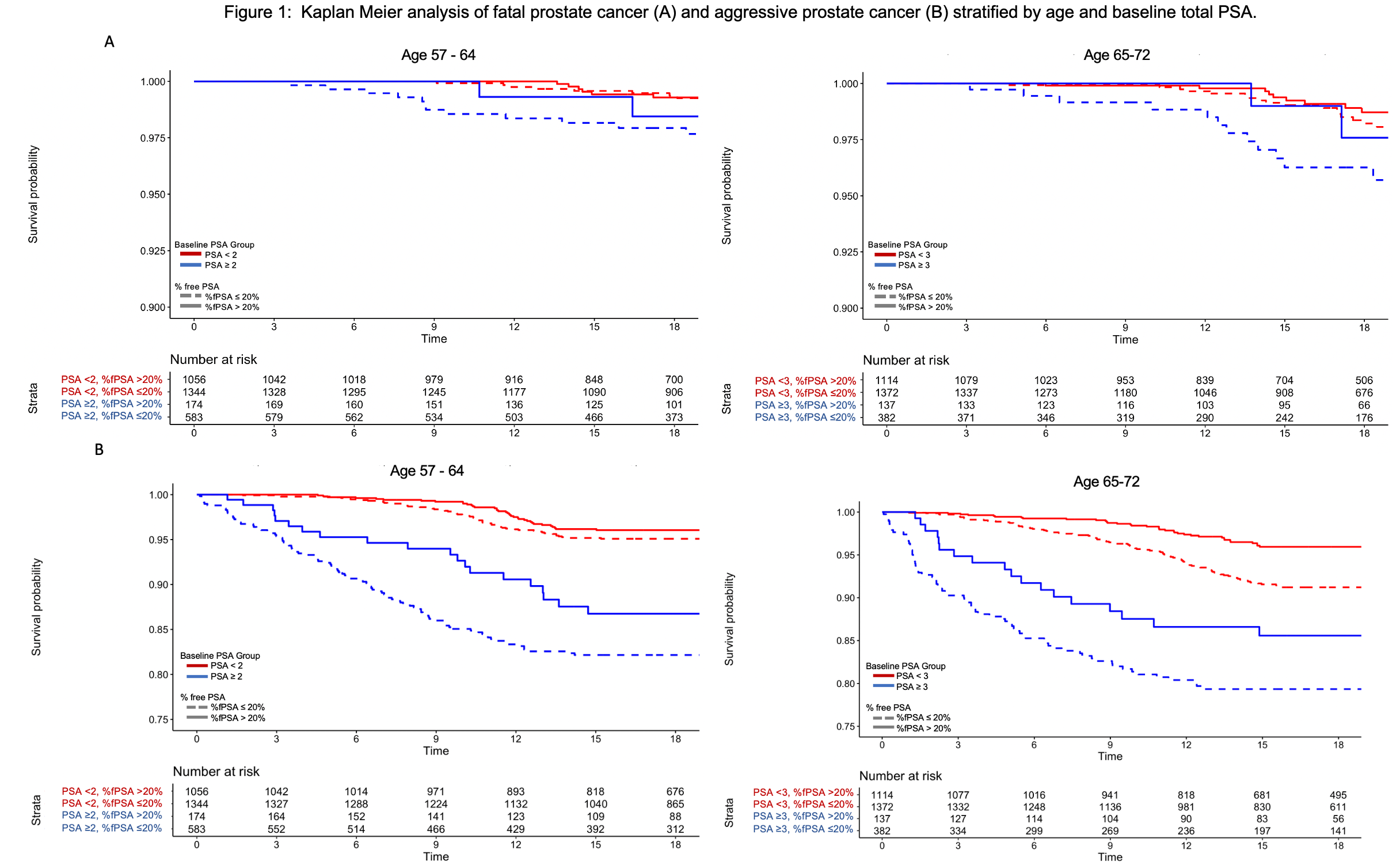
Introduction: We sought to determine if addition of free PSA (fPSA) to total PSA measured at baseline can improve prediction of clinically significant prostate cancer and fatal prostate cancer to guide risk-stratified screening. Methods: Of the 27,451 men in the intervention arm of the PCLO cancer screening trial, 6162 had a total PSA and fPSA measured within 1 year of randomization (defined as baseline). Patients were stratified into two age groups: 57-64 and 65-72 years. Clinically significant prostate cancer (csPCa) was defined as Gleason Grade =7, AJCC Stage >3, metastatic disease, or PCa death. Cumulative incidence and Kaplan-Meier analyses were conducted to estimate the probability of csPCa and fatal PCa and area under the curve (AUC) for discrimination. Results: Median follow up was 19 years during which 444 had csPCa and 92 had fatal PCa. Median PSA for overall cohort was 1.18 ng/mL, and median %fPSA was 18% at baseline. 75th percentile PSA levels were 3 ng/mL for ages 65-72 and 2 ng/mL for ages 57-64. In men 57-64 years with PSA=4 ng/mL and %fPSA >20%, the cumulative incidence (CI) of fatal PCa was 0.0/0.0% at 10/20 years and 2.1/3.0% for patients with %fPSA =20%. In men 65-72 years with PSA=5 ng/mL and % fPSA >20%, CI was 0.0/0.0% at 10/20 years and 1.4/6.3% for patients with %fPSA =20%. The predictive ability of total PSA for csPCa and fatal PCa was improved by adding %fPSA. In men 57-64 with PSA=2 ng/mL, AUC for fatal PCa increased from 0.55 to 0.69 by adding %fPSA and AUC for csPCa increased from 0.57 to 0.60. With PSA =3 ng/mL, AUC for fatal PCa increased from 0.41 to 0.65 with addition of %fPSA and AUC for csPCa increased from 0.57 to 0.64. In men 65-72 with PSA >4 ng/mL, AUC for fatal PCa increased from 0.63 to 0.65 by adding %fPSA and AUC for csPCa increased from 0.53 to 0.63. Kaplan-Meier curve (Fig 1) shows clear separation of curves for men with =20% fPSA compared to >20% fPSA in men with =75th percentile of total PSA at baseline. Conclusions: In a large nationwide screening trial, the addition of free PSA to total PSA in men with PSA >2 (age 57-64) or PSA > 3 (age 65-72) improved the prediction of clinically significant and fatal prostate cancer. The use of free PSA to risk-stratify screening could potentially decrease unnecessary prostate biopsies and be used to help determine when to terminate screening. SOURCE OF Funding: None