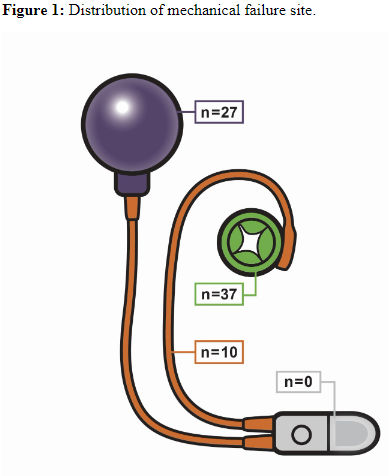
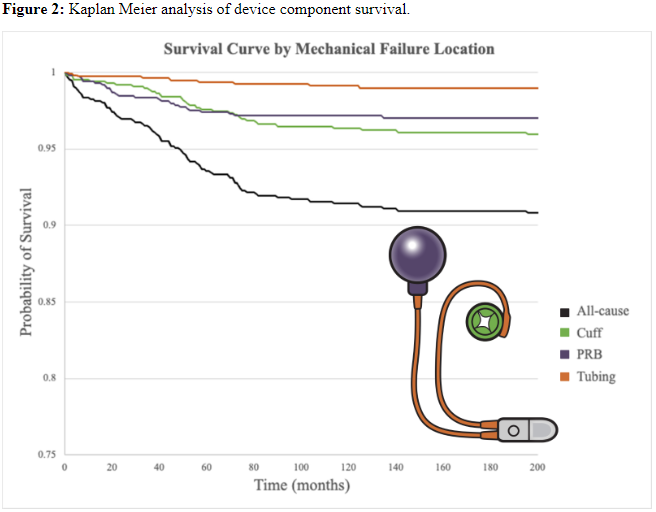
Introduction: Although the artificial urinary sphincter (AUS) remains the gold standard for severe stress incontinence, roughly half of patients require surgical revision for mechanical or non-mechanical reasons. We sought to delineate sites of mechanical failure in our high-volume tertiary referral center experience. Methods: A retrospective review of our AUS database from 2007–2021 was conducted to identify all men who had undergone AUS revision. Reason for revision was categorized as mechanical when attributed to failure at the pump, pressure regulating balloon (PRB), cuff, or tubing. Non-mechanical failures (e.g. infection, urethral erosion or atrophy) were excluded. Distribution and timing of component failure and patient characteristics were evaluated. Results: During the study period, 765 patients underwent 1059 AUS surgeries. Incidence of mechanical failure for virgin AUS implants was 9% (51/568) during the study period. Among 377 (35.6%) revision cases, 74 (19.6%) cases with clearly documented site of mechanical failure were included in this analysis. Half of mechanical failures were due to cuff leak (37/74, 50.0%); PRB failure was the next most common (27/74, 36.5%) (Figure 1). Tubing leaks were identified in ten cases (13.5%); no documented cases of pump failure were identified. Using a one-way ANOVA, there was no significant difference in mean time to failure between cuff (57.5 ± 43.9 months), PRB (33.7 ± 29.1 months), or tubing (50.3 ± 44.4 months) sites (p = .066). Other patient factors (age, BMI, ASA, and comorbidities) were similar between the three groups. Using a log-rank analysis, survival rates between cuff, PRB, and tubing failure groups were found to be statistically different, with poorest survival among cuff failures (?2=133.1, p < .001) (Figure 2). Conclusions: The predominant site of AUS device failure is the cuff, followed by the PRB. No instances of pump failure were identified over a nearly 15-year period. SOURCE OF Funding: N/A