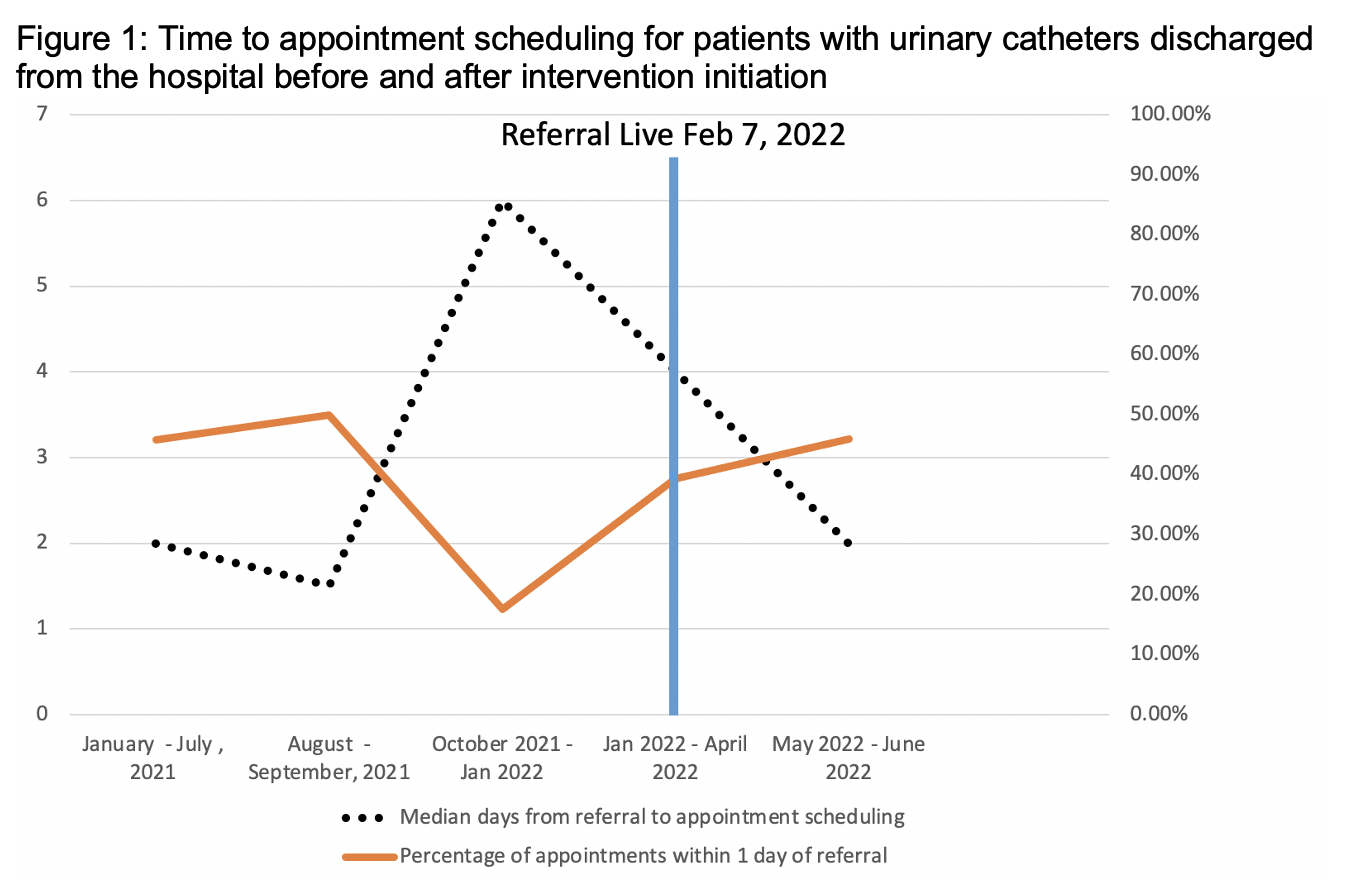
Introduction: Delays in patient care after discharge from the hospital can lead to poor quality care and outcomes. At UCSF, one source of patient discontinuity of care has been the inability to consistently obtain an expedited follow up appointment in the urology outpatient clinic after hospital discharge when patients had a new foley placed during their hospital stay. This quality improvement project sought to improve the process for these patients. Methods: To understand barriers to prompt follow up for patients discharging from UCSF, we employed LEAN A3 methodology. A total of 2 PDSA cycles were completed with two total interventions implemented. The first intervention was to create standing appointments with advanced practice providers that were reserved in the urology clinic for these discharge referrals. The second intervention was the creation of a novel patient self-scheduling approach using the existing electronic medical record. Patients who need referral for a voiding trial with urology were identified by their primary team and a new discharge order was placed. Placement of the referral order generated a ticket in the patient’s portal, allowing patients to select a date and time for their follow up voiding trial. Results: Prior to intervention, there was a median time of 2.0 days from referral placement to appointment scheduling and 9.5 days between referral placement and appointment date. (Figure 1) 20% of patients with referrals were lost to follow up. After the intervention, patients where were scheduled via the self-scheduling work flow had a median of 1.5 days from referral to scheduled appointment compared to 5.5 days from the prior work flow. The post intervention median time between referral placement and appointment scheduling was 8.0 days. 5% of patients in the post intervention period were lost to follow up. Conclusions: Automation and infrastructure enhancement improved the quality of care and shorted time to follow up for patients who had foley catheters placed during their hospital stay. Efforts like this can be scaled to improve urological quality of care and transitions in care. SOURCE OF Funding: none