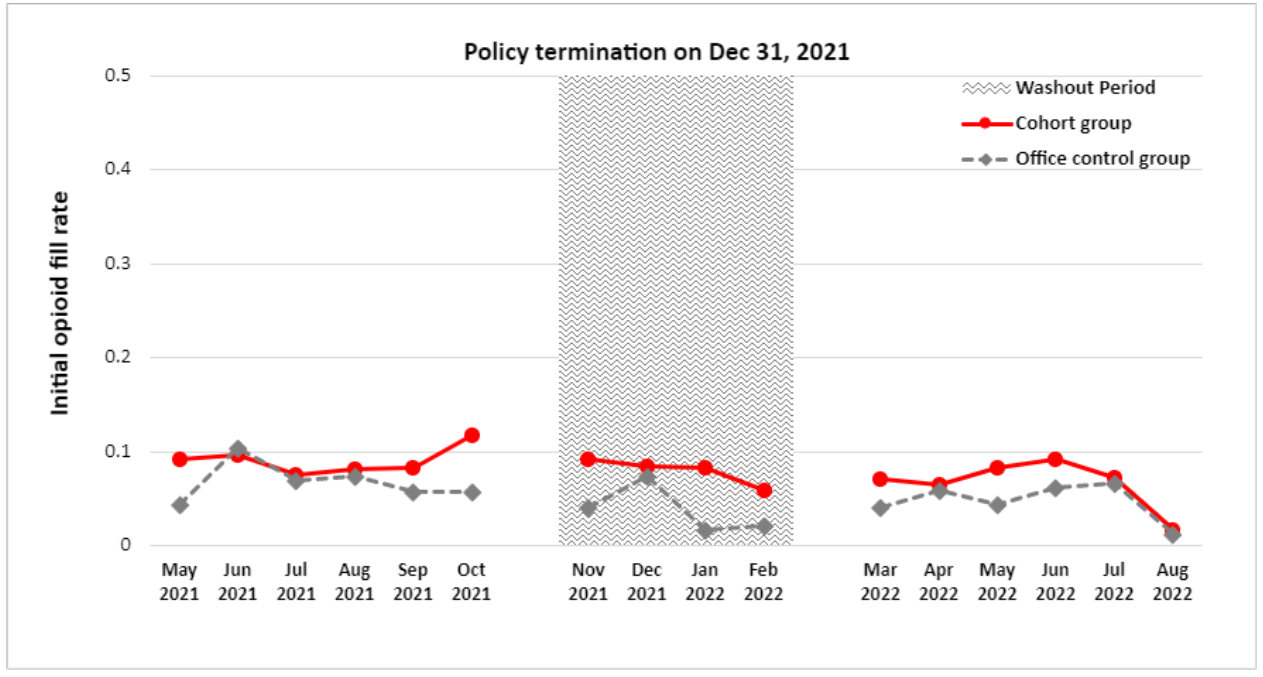
Introduction: Our prior work showed that financial incentive using modifier 22 by Blue Cross Blue Shield of Michigan (BCBSM) to encourage opioid-free vasectomy was associated with a significant decrease in initial opioid fills. However, this incentive was terminated on 12/31/21. We examined the change in initial opioid fill rate before and after termination of a quality incentive for opioid-free vasectomy. Methods: We analyzed BCBSM administrative claims from 5/1/2021 to 8/31/2022. We included men 20 to 64 years old undergoing an office-based vasectomy or a control procedure with continuous enrollment. Our control group included patients undergoing office circumcision, cystoscopy, prostate biopsy, and transurethral destruction of prostate tissue. We excluded cases 2 months before and after the policy termination date of 12/31/21 to account for variation in uptake. Our primary outcome was the proportion of patients, both opioid naïve and not, who filled an opioid prescription within 3 days of their procedure (aka, “opioid fill rate”). We performed an interrupted time series analysis to estimate changes in opioid fill rates before and after 12/31/21 in the vasectomy and control groups. Results: Our cohort included 2,209 who underwent vasectomy and 2,157 in the control group. Both groups had similar demographic and clinical attributes before and after 12/31/21, except the control group had statistically significant difference of smoking status and Charlson comorbidity score (p > 0.01) Termination of the modifier 22 policy was not associated with a change in the opioid fill rate in the vasectomy group (-0.6% change [95% CI: -6.5% to 5.3%]). (Figure 1) Pre-termination, 9.1% of men filled an opioid prescription; post-termination, 6.9% of men filled an opioid prescription. In the control group, the termination of the modifier 22 policy was not associated with a change in the opioid fill rate (-0.6% change [95% CI: -6.6% to 5.5%]). Conclusions: Financial incentives that support opioid-free pathways have led to a rapid decrease in the rate of opioid fills after vasectomy. Even following termination of this incentive, the low opioid fill rate was sustained. These findings highlight the opportunity for a modifier 22 quality incentive to be applied for a limited period to have sustainable impact in lowering opioid fill rate. SOURCE OF Funding: n/a