Vanderbilt University Medical Center, Nashville, TN
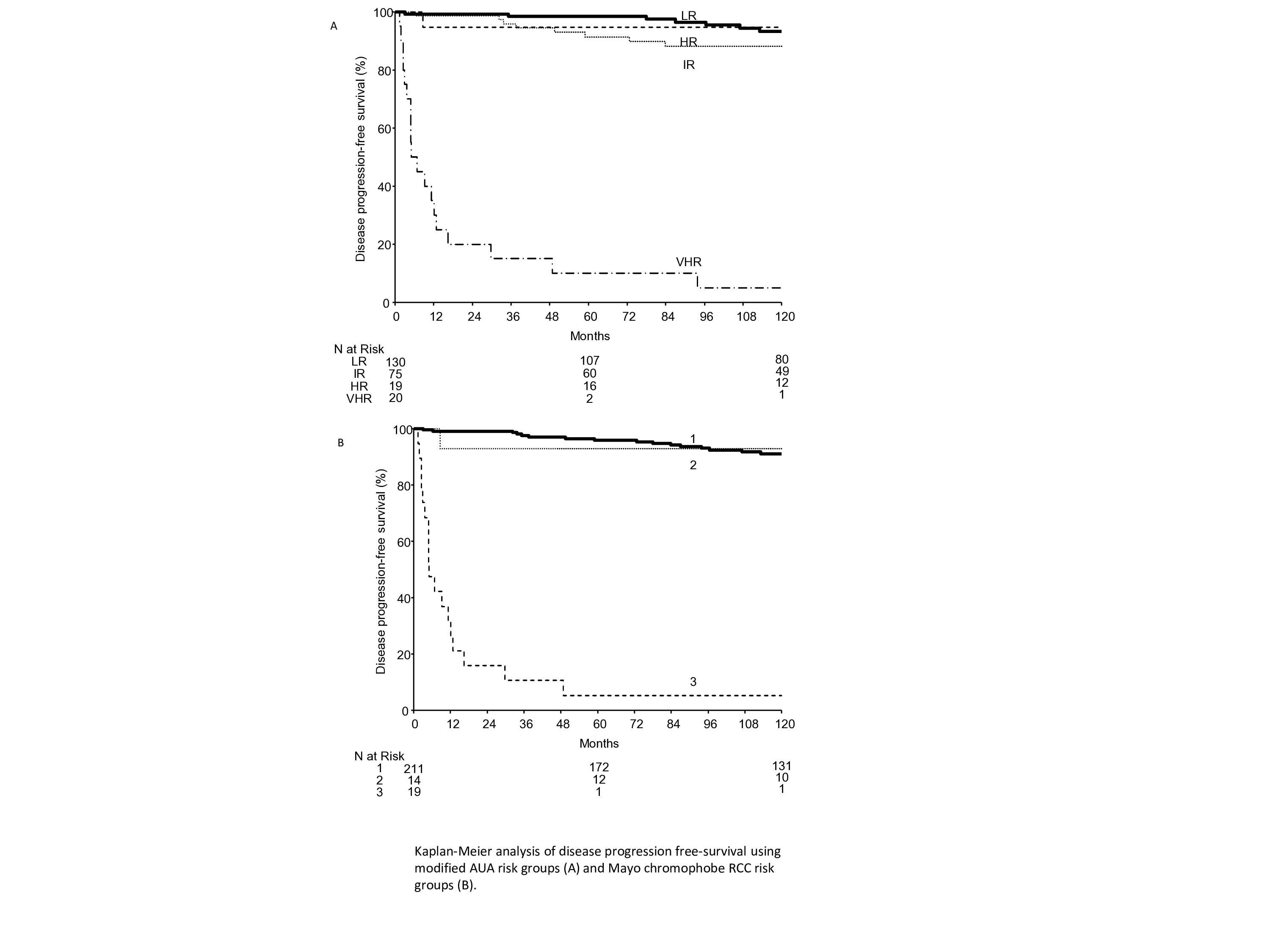
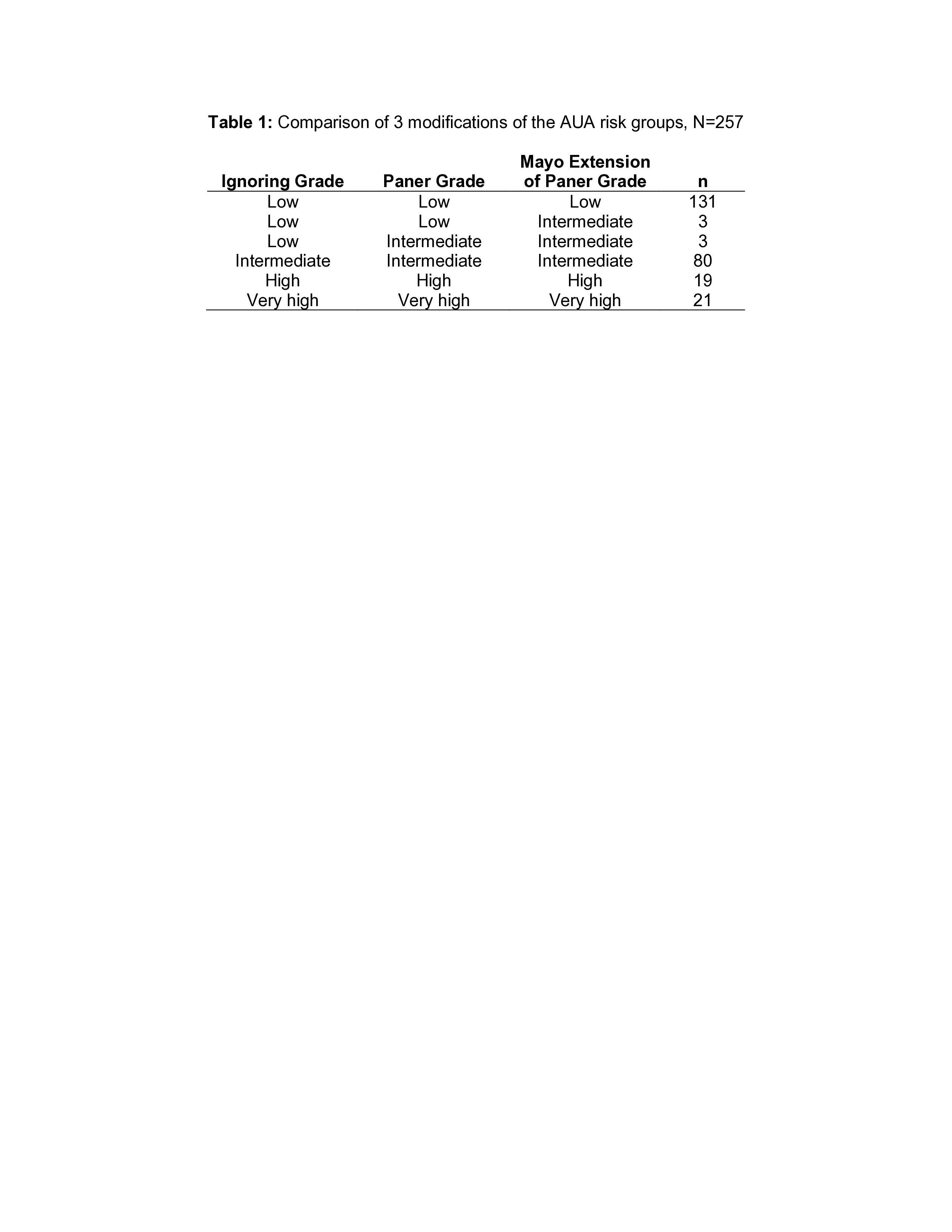
Introduction: In patients after surgery for localized renal cell carcinoma, prognostic models have been developed for progression-free (PFS) and cancer-specific survival (CSS). Notably, chromophobe RCC (chRCC) is unable to be classified by the American Urological Association (AUA) risk stratification system, as histologic grading of chRCC is not currently recommended. We sought to compare the Mayo risk stratification system (Leibovich 2018, Eur Urol) with three modified versions of the AUA RCC risk stratification system for chRCC. Methods: We queried the Mayo Clinic Nephrectomy Registry to identify patients treated with radical or partial nephrectomy for unilateral, sporadic, M0, chRCC from 1970 to 2012. AUA risk groups were defined using reported criteria excluding grade. Modified AUA risk groups included two proposed chRCC grading systems, including the Paner grading system and the Mayo extension of the Paner grade (Avulova 2021, Eur Urol). PFS and CSS were estimated using the Kaplan-Meier method. Predictive ability was summarized using c-indexes from Cox proportional hazard regression models. Results: A total of 257 patients with chRCC were identified. PFS and CSS rates at 120 months after surgery were 84% and 90%, respectively. PFS rates using AUA risk groups, ignoring grade, are summarized in Figure 1a, while PFS rates using the Mayo risk groups are presented in Figure 1b. C-indexes for AUA and Mayo risk groups were similar at 0.76 and 0.75, respectively, for PFS, and 0.77 and 0.76, respectively for CSS. Comparisons of the three modified AUA risk stratification systems with and without grading systems are presented in Table 1. Conclusions: The modified AUA and Mayo risk stratification systems have robust c-indexes for PFS and CSS in patients with chRCC. These models can be used to counsel patients based on the final pathologic analysis. Incorporation of proposed chRCC grading systems rarely results in re-stratification. SOURCE OF Funding: NA