Session: MP58: Kidney Cancer: Localized: Surgical Therapy III
MP58-04: Proposal and internal validation of a nomogram for the prediction of local recurrence free-survival after percutaneous ablation for cT1 renal masses
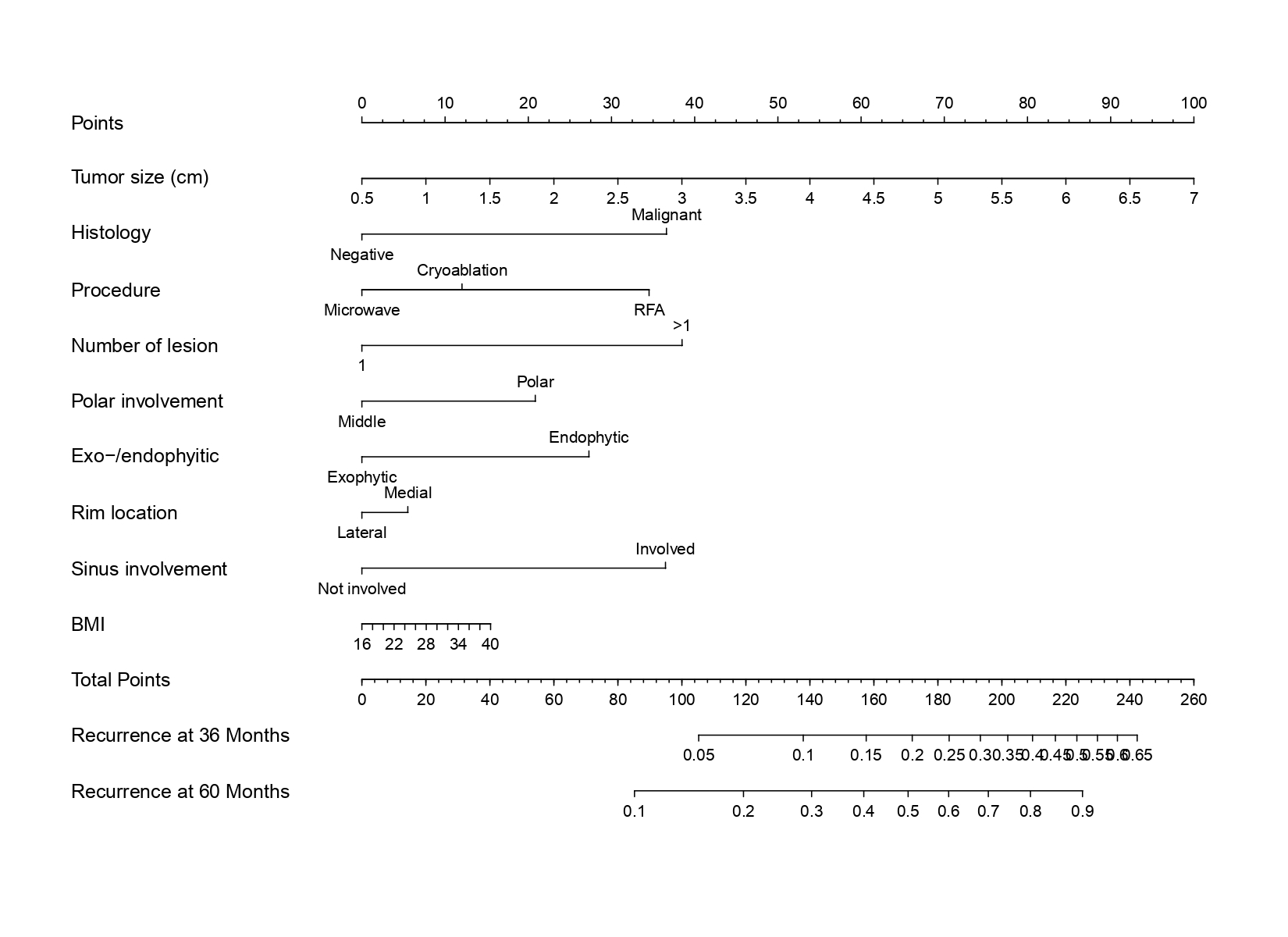
Introduction: Despite local tumor ablation (LTA) for the treatment of cT1 renal masses is increasing, the role of the different techniques used in influencing local recurrence is still unclear. We aim to develop a nomogram predicting local recurrence-free survival after different type of percutaneous LTA for small renal masses. Methods: We identified 433 patients who underwent percutaneous LTA with radiofrequency (RFA), cryoblation (Cryo) or microwave (MW) ablation at four tertiary referral centers for cT1 renal masses. All patients received a biopsy of the mass before treatment. Patients’, as well as renal masses’ characteristics were collected. The primary end point was local recurrence. Statistical analyses consisted of two steps. First, a nomogram predicting local recurrence was built relying on multivariate Cox regression analysis. Second, performance characteristics of the nomogram were assessed at a threshold of 60 months, and compared to model exclusively based on clinical size and tumor’s histology, using Heagerty’s C and decision curve analysis (DCA). Results: Overall, 393 (90.8%) patients had a positive biopsy for renal cancer while 40 (9.2%) patients had an undetermined biopsy. Overall, 172 (39.7%), 123 (28.4%), 138 (31.9%) patients underwent Cryo, MW and RFA, respectively. No differences in terms of age, CCI, BMI, clinical size (cm) and histology at pre-ablative biopsy were recorded among the three groups (all p>0.05). Overall, 53 patients (12.2%) recurred after a median time of 34 (IQR 18-60) months. The nomogram relied on the following variables: tumor size (cm), histology (malignant or undetermined), type of ablative procedure (MW, Cryo or RFA), polar involvement, >50% vs =50% exophytic rate, rim location (lateral or medial), sinus involvement and BMI. The newly developed nomogram yielded an area under the curve of 0.82 vs 0.73 for the model based on clinical size and histology. Moreover, the new nomogram also exhibited greater net-benefit across all threshold probabilities at DCA (Fig 1). Conclusions: The proposed nomogram to predict local recurrence after different techniques of LTA for renal cancer provides valuable information for both patient’s and technique’s selection for focal ablation of renal masses. SOURCE OF Funding: no

.jpg "Angelo Mottaran, MD photo")