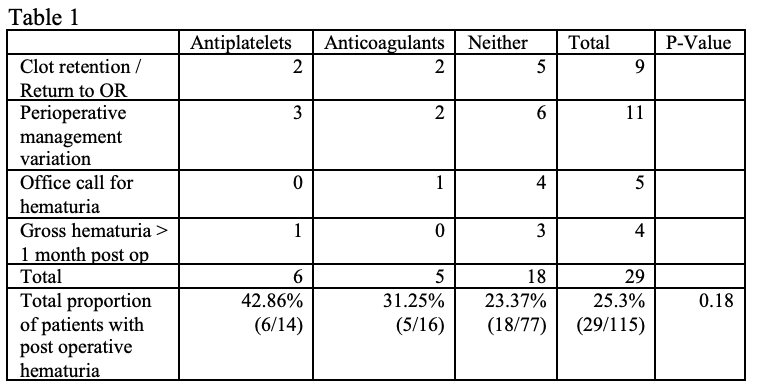
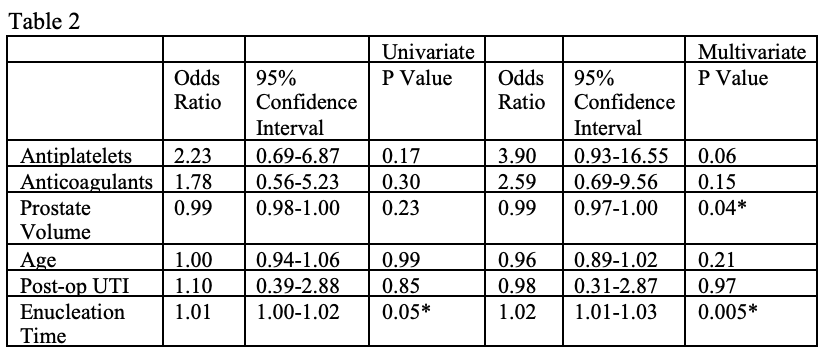
Introduction: Holmium enucleation of the prostate (HoLEP) is offered for symptomatic prostatic enlargement at high risk for bleeding. However, prior studies define clinically significant hematuria (CSH) narrowly as return to operating room or need for transfusion. We sought to evaluate risk factors contributing to a broader definition of CSH which may contribute to alteration of clinical course. Methods: We retrospectively analyzed 115 patients who underwent HoLEP at a single institution across two surgeons from November 2020 to October 2022. HoLEP was performed using Moses 2.0 (Boston Scientific) laser and the Piranha enucleation system (Richard Wolf). We defined CSH broadly: clot retention, return to operating room, perioperative management variation due to hematuria, office calls for hematuria, or continued gross hematuria past one month post operatively. Pearson Chi-squared, univariable and multivariable analysis were used where appropriate. Multivariable analysis of CSH risk based on use of antiplatelet agents or anticoagulants included correction for age, enucleation time (surrogate for case difficulty), post-operative urinary infection, and prostate volume. Results: 25.3% (29/115) of our patients developed CSH after HoLEP. 42.86% of patients on antiplatelets and 31.25% on anticoagulants had significant hematuria, compared to 20.78% on neither (P = 0.18). Longer enucleation time was a risk factor for developing CSH (Univariate OR 1.01, p=0.05). Neither antiplatelets nor anticoagulants were a risk factor (P=0.17; P=0.30). Conclusions: With a broadened definition, 25% of patients developed CSH following HoLEP, which impacted the clinical course. Our data suggests that the current definition of significant hematuria is too narrow and does not capture many patients whose clinical course is affected by hematuria. While longer enucleation time was a risk factor for developing CSH hematuria, we found no difference in CSH with patients on antiplatelets or anticoagulants compared to controls, though larger studies are needed. SOURCE OF Funding: n/a