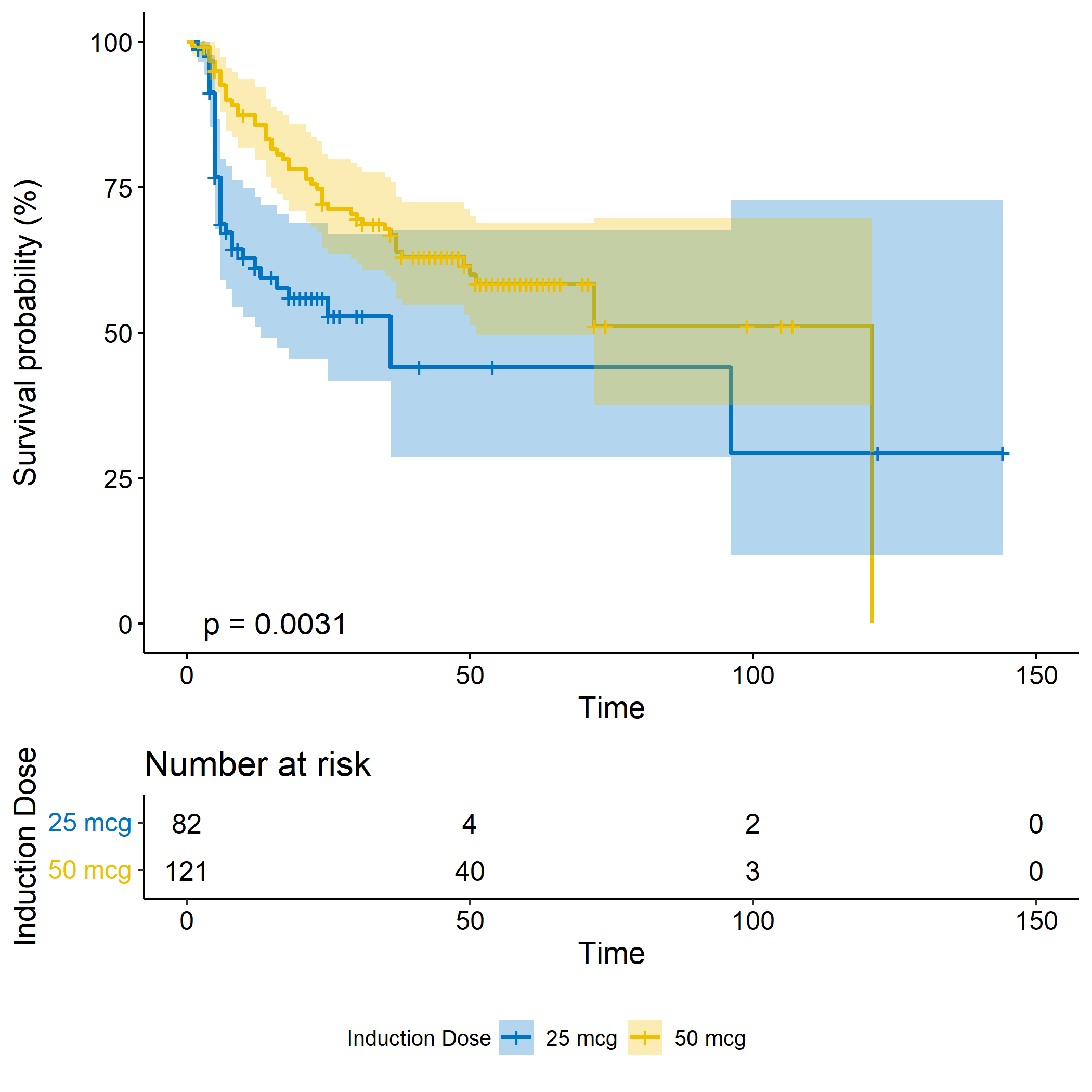
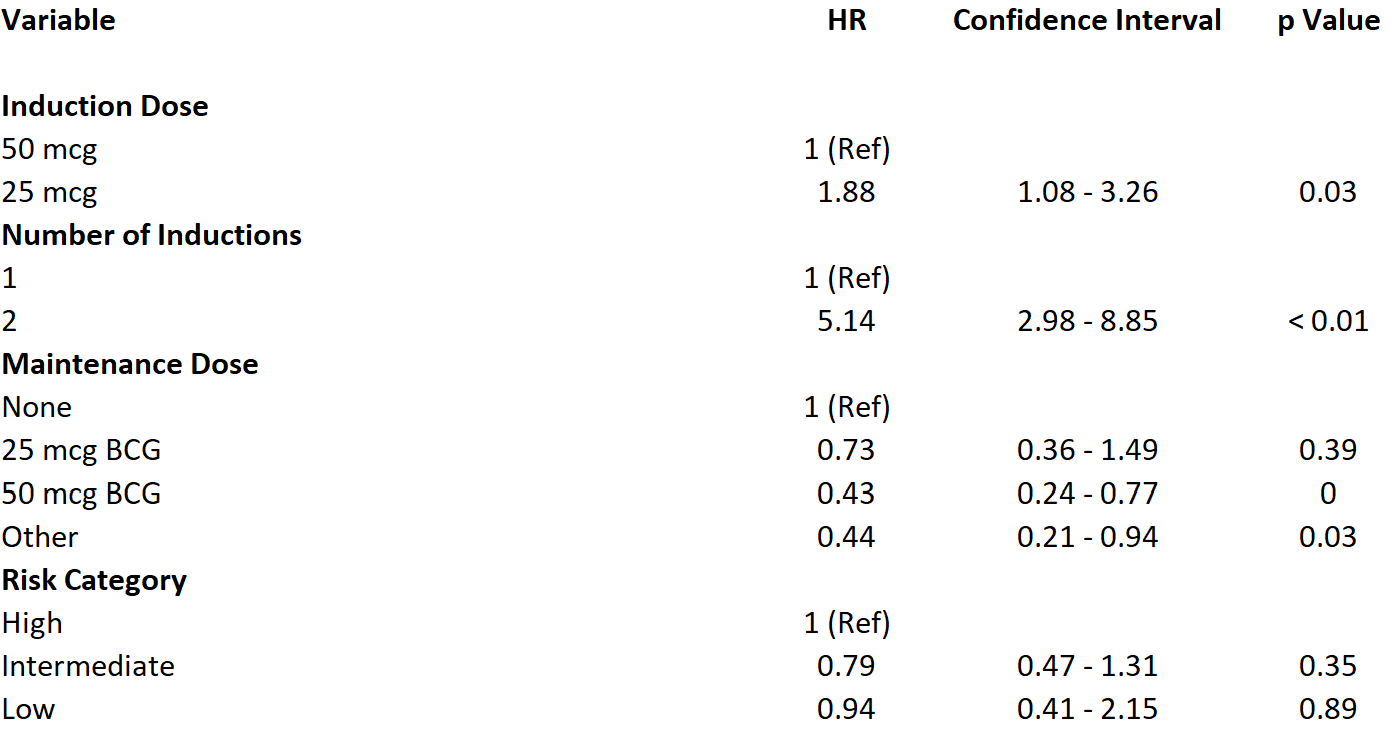
Introduction: The BCG shortage era has prompted the need for rethinking of the classic treatment paradigm for non-muscle invasive bladder cancer (NMIBC). Among other approaches, reduced BCG dosage protocols have been implemented across various institutions with conflicting evidence on their efficacy. We retrospectively evaluated patients at out institution with NMIBC and hypothesized that reduced dose protocols would have no significant impact on the development of BCG-relapsing disease, BCG-refractory disease, or progression to muscle invasive bladder cancer. Methods: We evaluated 300 patients treated at our institution during the BCG shortage era (01/2017 – 05-2021). After obtaining institutional IRB approval, we retrospectively reviewed the charts of 300 patients and recorded pathology at diagnosis, size of tumor at initial resection, BCG induction dose (25 mg vs. 50 mg), BCG maintenance dose (25 mg vs 50 mg), pathology and date of recurrence. We evaluated baseline differences between full and reduced dose groups utilizing chi-squared tests, t-test, and ANOVA where appropriate. We then compared time to recurrence between the two dosing strategies with log-rank tests and Cox proportional hazards models. Results: 203 patients with complete data were treated with BCG during the period of the study (115 high risk, 73 intermediate risk). Patients who received a lower induction dose of were more likely to develop a recurrence during the study period (log-rank test, p < 0.001, Figure 1). On multivariable Cox proportional-hazards modelling, those who received reduced dose BCG were more likely to experience a recurrence during the study period (HR: 1.88, 95% CI 1.08 – 3.26) while adjusting for number of inductions, maintenance dosing, and AUA risk category. Conclusions: In this cohort of mainly high-risk NMIBC patients, those treated with reduced induction dose of BCG were more likely to experience a recurrence within the study period. Additional research and prospective trials can shed light on which patients are able to safely be treated with reduced dose BCG in the shortage era. SOURCE OF Funding: Institutional funding.