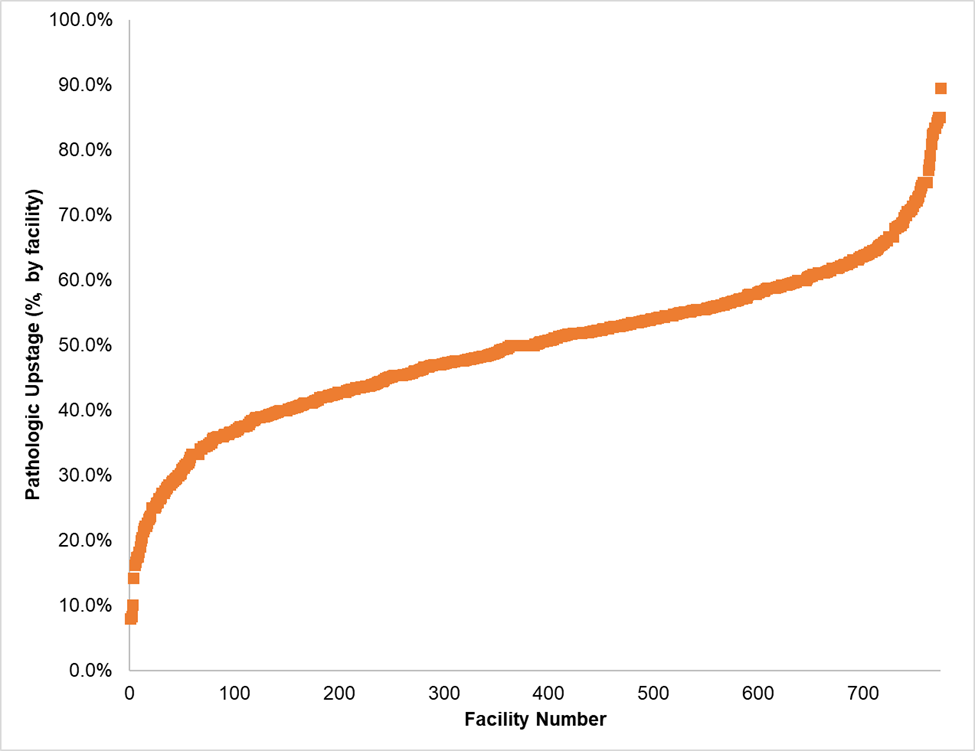
Introduction: The rate of bladder cancer pathologic upstaging at the time of radical cystectomy (RC) is estimated to be as high as 40% and has been associated with worse survival. Prior studies have examined patient and disease specific factors. The aim of this study is to determine the impact of treatment facility and facility level factors on upstaging of bladder cancer at the time of RC. Methods: Data from the National Cancer Database was used to conduct this retrospective analysis. We identified patients between 2004 and 2019 with urothelial cancer who underwent RC. The primary outcome was pathologic upstaging defined as an increase in pathologic T or N stage when compared to the clinical T or N stage. Variation across facilities and facility-specific factors associated with high pathologic upstaging were measured using descriptive analyses. Shared frailty modeling, which includes neoadjuvant treatment as a covariate, was used to describe the relationship between pathologic upstaging and survival. Results: 64,675 patients were treated at 774 facilities and were included in this analysis. Of these, 17,961 (27.8%) received care at more than one Commission on Cancer-accredited facility. A total of 32,142 patients (49.7%) were upstaged following RC with 41.2% (26,657) upstaged T stage and 17.6% (11,395) upstaged N stage. Rate of upstaging varied by treating facility, from 0.8% - 89.5% (median 50.2% [IQR 42.4 - 57.0%]). Hospitals were divided into quintiles based on rate of upstaging: very low (0.8 - 40.4%, N=155), low (40.5 - 47.6%, N=155), medium (47.6 - 52.9%, N=158), high (53.0 - 59.1%, N=153), very high (59.3 - 89.5%, N=153). Low volume (OR 2.6, 1.5 - 4.5, P<.001) and non-academic facilities (OR 2.2, 1.4 - 3.6, P=.001) were associated with very high rates of upstaging. Following adjustment for initial clinical stage, patient characteristics, and clinical factors, upstaging was associated with decreased survival (HR 2.10 [2.05 - 2.16], P<.001). Conclusions: The rate of bladder cancer upstaging after RC varies considerably across treatment facilities and is associated with decreased survival. Ensuring that patients have access to care at facilities with high case volume and other factors associated with decreased rates of upstaging are potential means to improving survival. SOURCE OF Funding: None