Northwestern University - The Feinberg School of Medicine
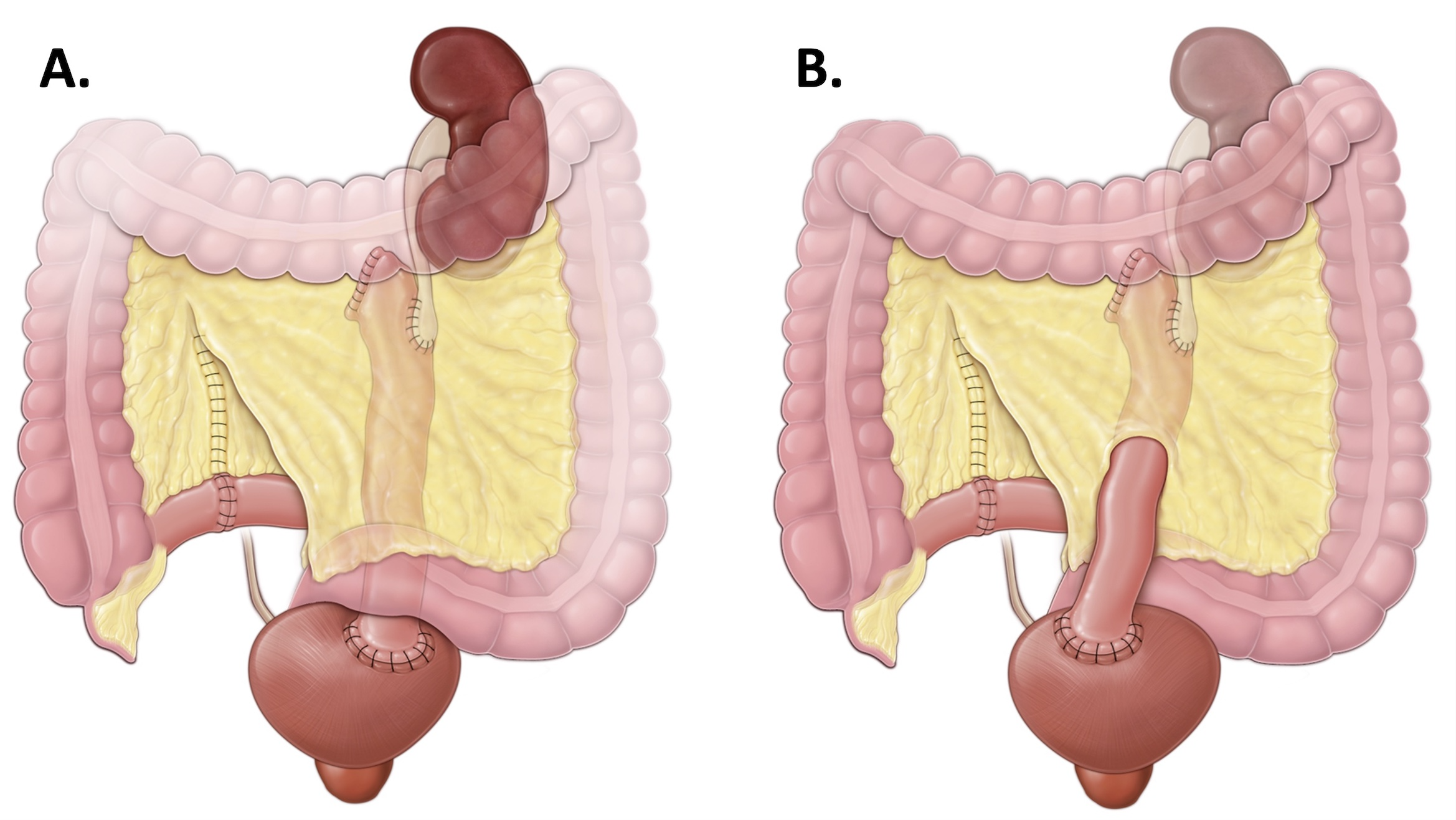
Introduction: Intracorporal robotic left ileal ureter replacement is a technically challenging procedure. Only a handful of reports exist in the literature. We describe our approach for intracorporal robotic left ileal ureter replacement and highlight key aspects of our surgical technique. Methods: We demonstrate our technique on a 49-year-old woman with a 25-centimeter left pan-ureteral obliteration secondary to endoscopic stone surgery. Our technique involves five major steps: proximal ureteral dissection, bowel harvest, bladder dissection, distal anastomosis, and proximal anastomosis. In order to optimize access to the upper and lower urinary tracts, we use two distinct patient positions and port placement schemas based on the field of interest. Tilting the bed allows for toggling between the modified flank (upper tract) and modified supine positions (lower tract) without the need to reposition or redrape the patient. During reconstruction, the ileal ureter may be brought over to the left side by tunneling only the proximal segment or by tunneling the entire segment of ileum (Figure 1). Results: For our index case, operative time was 340 minutes, estimated blood loss was 200 milliliters, and length of stay was 5 days. There were no 90-day major postoperative complications. Renal scan obtained at 4 months postoperatively demonstrated a T1/2 of 14 minutes. At 8 months follow-up there was no evidence of stricture recurrence. Conclusions: Intracorporal robotic left ileal ureter replacement is a reproducible technique for the management of pan-ureteral stricture disease. Adhering to a system and simplifying the technique into five steps may facilitate successful completion of this challenging procedure. SOURCE OF Funding: None

 photo")