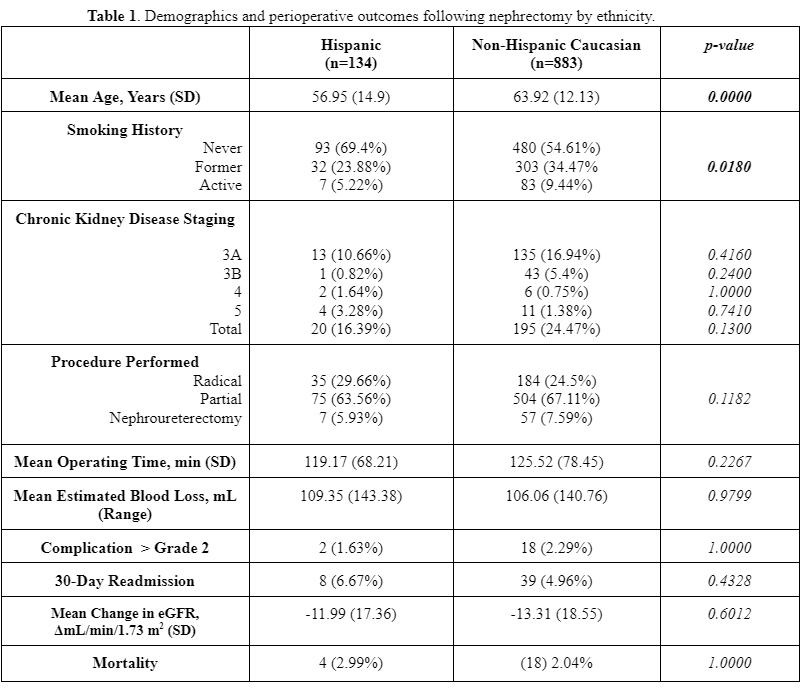
Introduction: We aim to determine if Hispanic patients differed in clinical presentation and surgical management of renal masses compared to Non-Hispanic Caucasian patients in our Northern New Jersey catchment area. Methods: We utilized an IRB-approved renal mass database including 1017 patients who underwent partial or radical nephrectomy at our institution between May 2017 and April 2022. We evaluated 1017 patients who identified as either “Hispanic” or “Non-Hispanic Caucasian.” Continuous data was analyzed using the Wilcoxon Rank Sum test. Categorical data was analyzed using Chi-Squared and Fisher's Exact Tests where appropriate. Results: 134 patients (13.18%) self-identified as Hispanic and 883 (86.82%) identified as Non-Hispanic Caucasian (Table 1). In terms of presentation, Hispanic patients were significantly younger on average (56.95 vs 63.92, p=0.0000), more likely to be female (48.51% vs 33.64%, p=0.0001), and less likely to have a history of tobacco use (29.10% vs 43.57%, p=0.018). Hispanic patients had lower incidences of coronary vascular disease (1.491% vs 6.0%, p=0.0315) and chronic kidney disease prior to undergoing surgery (16.39% vs 24.47%, p=0.0158). There was no significant difference in rates of undergoing radical nephrectomy between the two groups (29.66% vs 24.5%, p=0.6212). There was no significant difference in changes from baseline preoperative eGFR (-11.99 vs -13.31 mL/min/1.73 m², p=0.6012). Additionally, there was no significant difference in the rate of major complications (1.63% vs 2.29%, p=1.0), readmissions (6.67% vs 4.96%, p=0.4328), or mortality (2.99% vs 2.27%, p=1.000). Conclusions: In our Northern New Jersey population, we found that Hispanic patients presented with renal masses at younger ages with less comorbidities and less prior tobacco use in comparison to Non-Hispanic Caucasian patients. We did not identify significant differences in surgical management, perioperative or long-term outcomes between these cohorts. Our findings suggest that high volume, quaternary medical centers may reduce inequalities in access to care for patients from ethnic minorities. SOURCE OF Funding: No funding.

 photo")