MP43-05: Testicular Sperm Aspiration (TESA) vs. Microfluidic Sperm Separation (MSS) in Couples with High Sperm DNA Fragmentation Undergoing ICSI: Which Approach is Better?
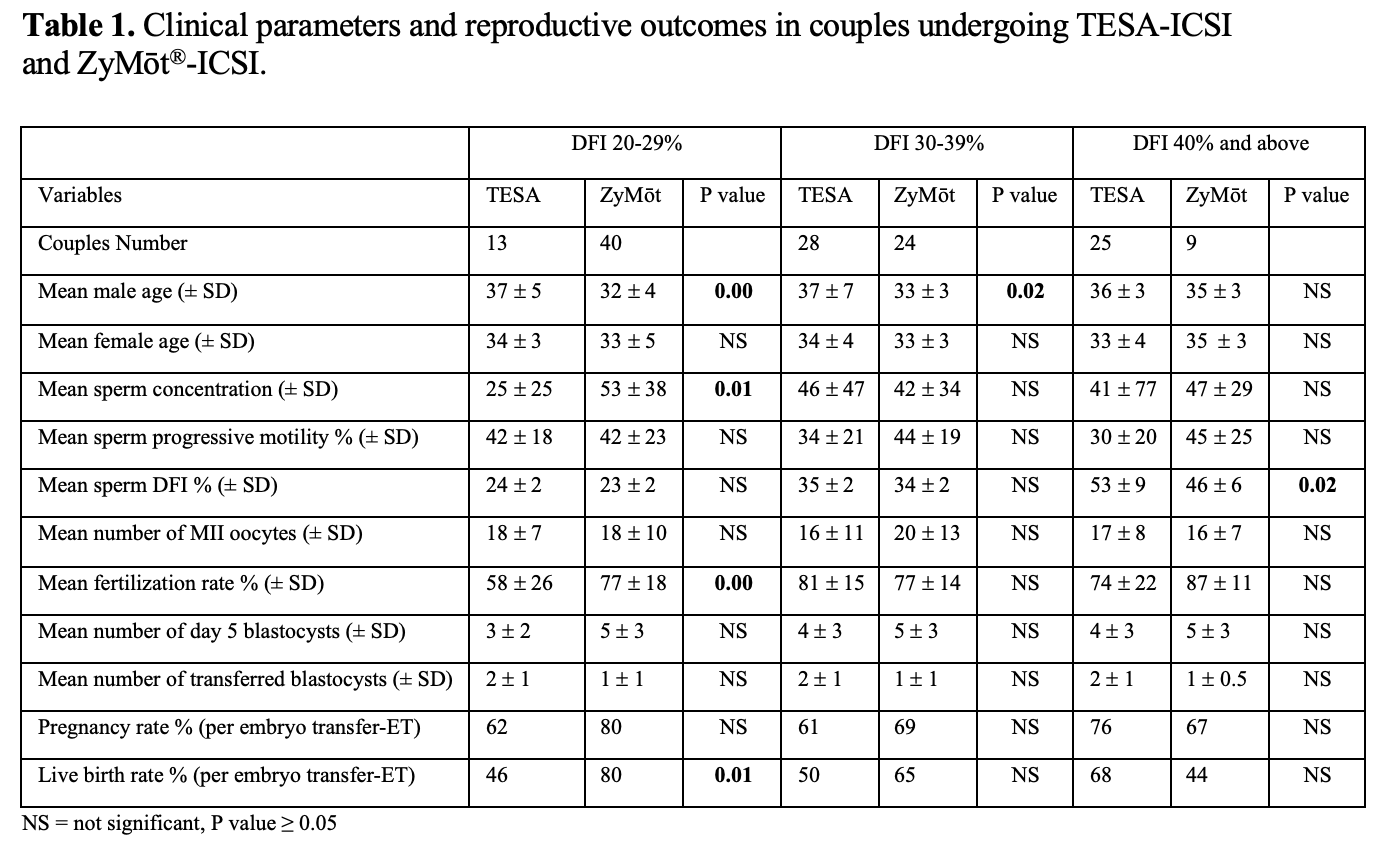
Introduction: Testicular sperm aspiration (TESA) and microfluidic sperm separation (MSS) are modalities designed to select the best sperm quality for intra-cytoplasmic sperm injection (ICSI) in men with poor sperm DNA integrity. We sought to investigate and compare reproductive outcomes in couples with a high sperm DNA fragmentation index (DFI) using TESA-ICSI or MSS-ICSI. Methods: We conducted a retrospective study of consecutive infertile couples with high DFI who underwent ICSI using TESA, or MSS. Couples were divided into 3 subgroups based on sperm DFI results (20-29%, =30-39% and =40% DFI). Sperm DFI was determined by flow cytometry based TUNEL assay (terminal deoxynucleotidyl transferase-mediated dUTP nick end-labeling). We utilized the ZyMot® microfluidic sperm selection device. We excluded cycles with advanced maternal age (> 40 years) and included cycles with transfer of day 5 blastocysts. Results: After excluding cycles with advanced maternal age and those that did not proceed to day 5 blastocyst transfer, we identified 66 couples in the TESA cohort and 73 couples in the MSS cohort. Maternal age was not significantly different in the TESA vs. the MSS cycles in any of the DFI subgroups. However, paternal age was significantly higher in the TESA than in the MSS cycles within the 20-29% and 30-39% DFI subgroups (Table 1). There were no significant differences in pregnancy rates per embryo transfer in any of the DFI subgroups, However, live birth rates were higher in the MSS vs. the TESA cycles in the 20-29% DFI group. A trend toward higher live birth rates in the TESA vs. MSS cycles in the =40% DFI subgroup was noted (Table 1). Conclusions: TESA-ICSI and MSS-ICSI offer similar pregnancy rates per embryo transfer in couples with high DFI although MSS may be a better option than TESA in terms of live birth rates in couples with DFI in the 20-29% range. Larger studies are needed to define the optimal use of these sperm selection modalities in the treatment of couples with high DFI. SOURCE OF Funding: None.