MP46-11: Long-term oncologic outcomes of robot-assisted radical cystectomy: update series from a high-volume robotic center beyond 10 years of follow-up
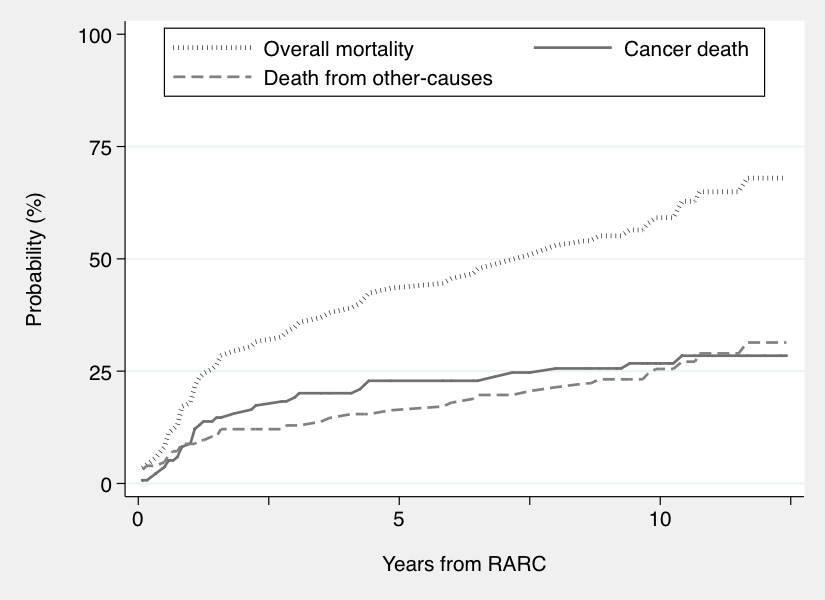
Introduction: Long-term oncologic data on patients undergoing robot-assisted radical cystectomy (RARC) for non-metastatic bladder cancer (BCa) are limited. We here assessed long-term oncologic outcomes of patients receiving robotic radical cystectomy at a high-volume European Institution. Methods: We analyzed data of 107 patients treated with RARC between 2003 and 2012 at a high-volume robotic center (OLV Hospital, Aalst, Belgium). All surgeries were performed by two high-volume surgeons. Clinical, pathologic, and survival data at the latest follow-up were collected. Clinical recurrence (CR)-free survival, cancer-specific mortality (CSM)-free survival, and overall survival (OS) were plotted using Kaplan-Meier survival curves. Cox proportional hazards models investigated predictors of CR and CSM. Competing risk regressions were utilized to depict cumulative incidences of death from BCa and death from other causes after RARC at long-term. Results: Pathologic nonorgan-confined BCa was found in 40% of patients, and 7 (7%) patients had positive soft tissue surgical margins. Median (interquartile range [IQR]) number of nodes removed was 11 (6, 14), and 26% of patients had pN+ disease. Median (IQR) follow-up for survivors was 123 (117, 149) months. The 12-year CR-free, CSM-free and overall survival were 55% (95% confidence interval [CI]: 44%, 65%), 62% (95%CI: 50%, 72%), and 34% (95%CI: 24%, 44%) respectively. On multivariable competing risk analysis, nodal involvement at final pathology was associated with higher risk of both CR (hazards ratio [HR]: 1.82; 95%CI: 1.06, 3.13, p=0.030) and CSM (HR: 1.70, 95%CI 1.30, 2.22; p<0.0001). The cumulative incidence of non-cancer death exceeded that of death from BCa after approximately ten years after RARC (Figure 1). Conclusions: We provided relevant data on the oncologic outcomes of RARC at a high-volume robotic center, with acceptable rates of clinical recurrence and cancer-specific survival at long-term. In patients treated with RARC, the cumulative incidence of death from causes other than BCa is non-negligible, and should be taken into consideration for post-operative follow-up. SOURCE OF Funding: None