MP46-18: Spectrum and Incidence of Urinary Tract Infections (UTI) in patients undergoing Radical Cystectomy: Results from a single center study and Proposal for ERAS protocol
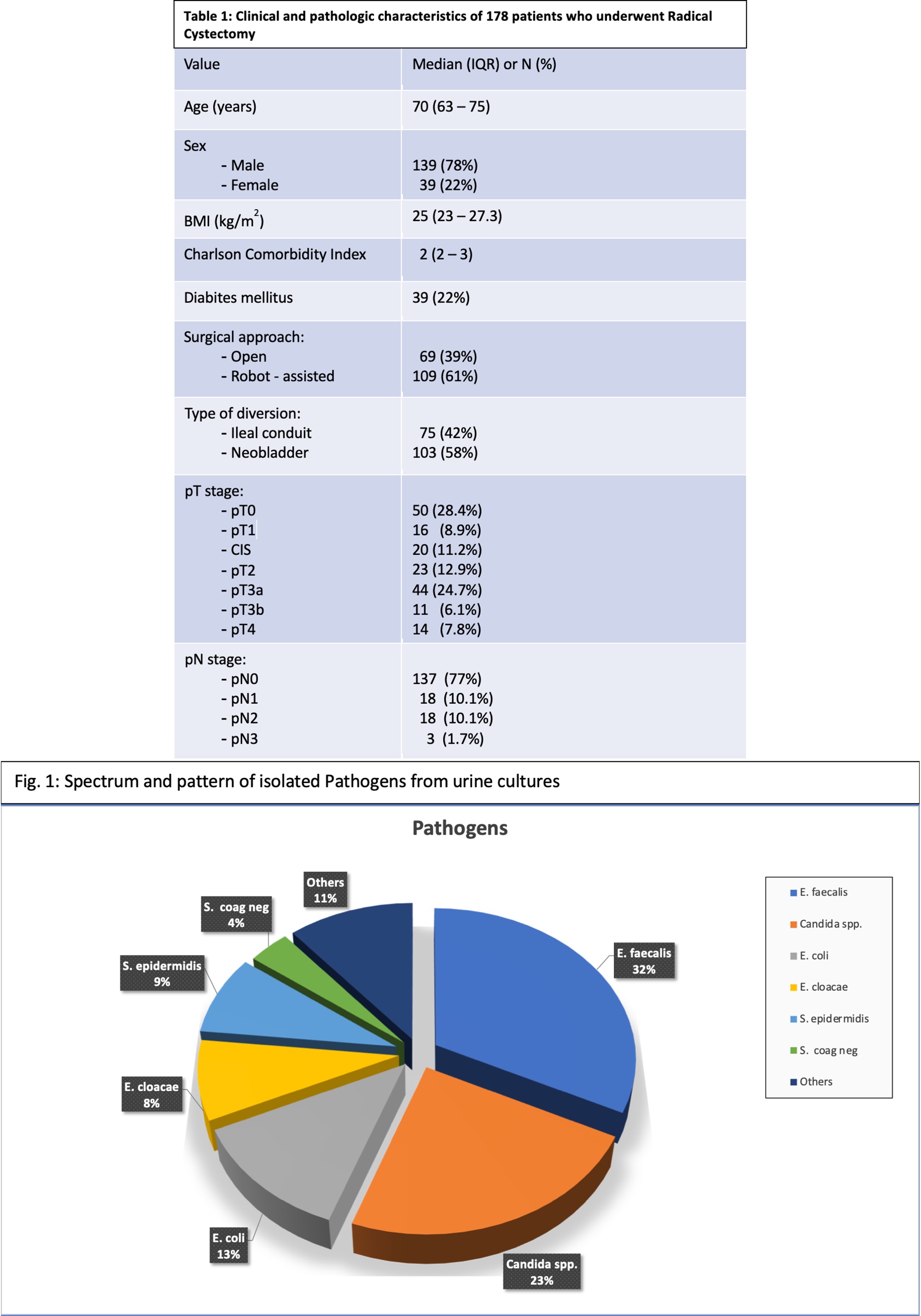
Introduction: Radical cystectomy (RC) has a high rate of postoperative complications. Our aim was to assess the spectrum of UTI and efficacy of our ERAS protocol. Methods: We analyzed prospectively collect data from 206 patients (Pts) undergoing RC at our Institution from 2015 to 2020. A fully comprehensive ERAS protocol was applied. Urine cultures (UCs) were taken before surgery and Pts treated accordingly. One-shot intraoperative antibiotic (ABT) prophylaxis was used. UCs were collected from urinary drains (UD) at POD 4. Pts with positive UCs and Ileal conduit (IC) were not treated if asymptomatic whilst all Neobladder (NB) pts with positive UCs received ABT based on reports till complete removal of UDs (POD 10). Pts with NB and negative UCs received short-term ABT 24h prior and after neobladder catheter ablation. Rate of in-hospital UTIs was recorded, differentiated and defined as Systemic inflammatory Response Syndrome (SIRS) and Sepsis (SEP) according to Sepsis-3 Consensus Definitions. Results: Clinicopathological characteristics are in Table 1. Pathogens are shown in Figure 1. Overall, 17/178 (9.4%) of Pts experienced SIRS, 18/178 (9.9%) sepsis whilst the remainder 147/178 (80.7%) did not have any UTI. In the IC group, occurred 7/75 (9.3%) and 8/75 (10.7%) cases of SIRS and SEP respectively. In same group, 56/75 (74.5%) had bacteriuria, of them 32/75 (57%) did not receive ABT as per protocol, resulting in only 1/75 (1%) case of UTI-SIRS. There was no significant difference in rate of SIRS (p=0.6) and SEP (p=0.4) in pts with UC+ and UC- for IC Pts. In the Neobladder (NB) group, there were 10/103 (9.7%) and 10/103 (9.7%) of SIRS and SEP respectively. 81/103 (78.6%) of NB pts had bacteria in at last one UD. There was no significant difference in rate of SIRS (p=0.6) and SEP (p=0.3) in Pts with UC+ and UC- for NB patients. No statistically significant difference (p>0.5) was observed in both groups in the rate of UTI considering surgical approach (Open vs Robotic). Conclusions: UTI-related complications represent a challenge after RC. Our protocol is safe and effective to maintain the rate of UTIs low allowing for effective use of ABT according to the principles of antimicrobial stewardship and ERAS. Our protocol seems to be effective for both urinary reconstructions. SOURCE OF Funding: None

 photo")