Session: MP48: Health Services Research: Practice Patterns, Quality of Life and Shared Decision Making II
MP48-08: 30-day, 90-day, and 1-year complications following major urologic surgery: an analysis of morbidity and mortality using a large multi-center research network
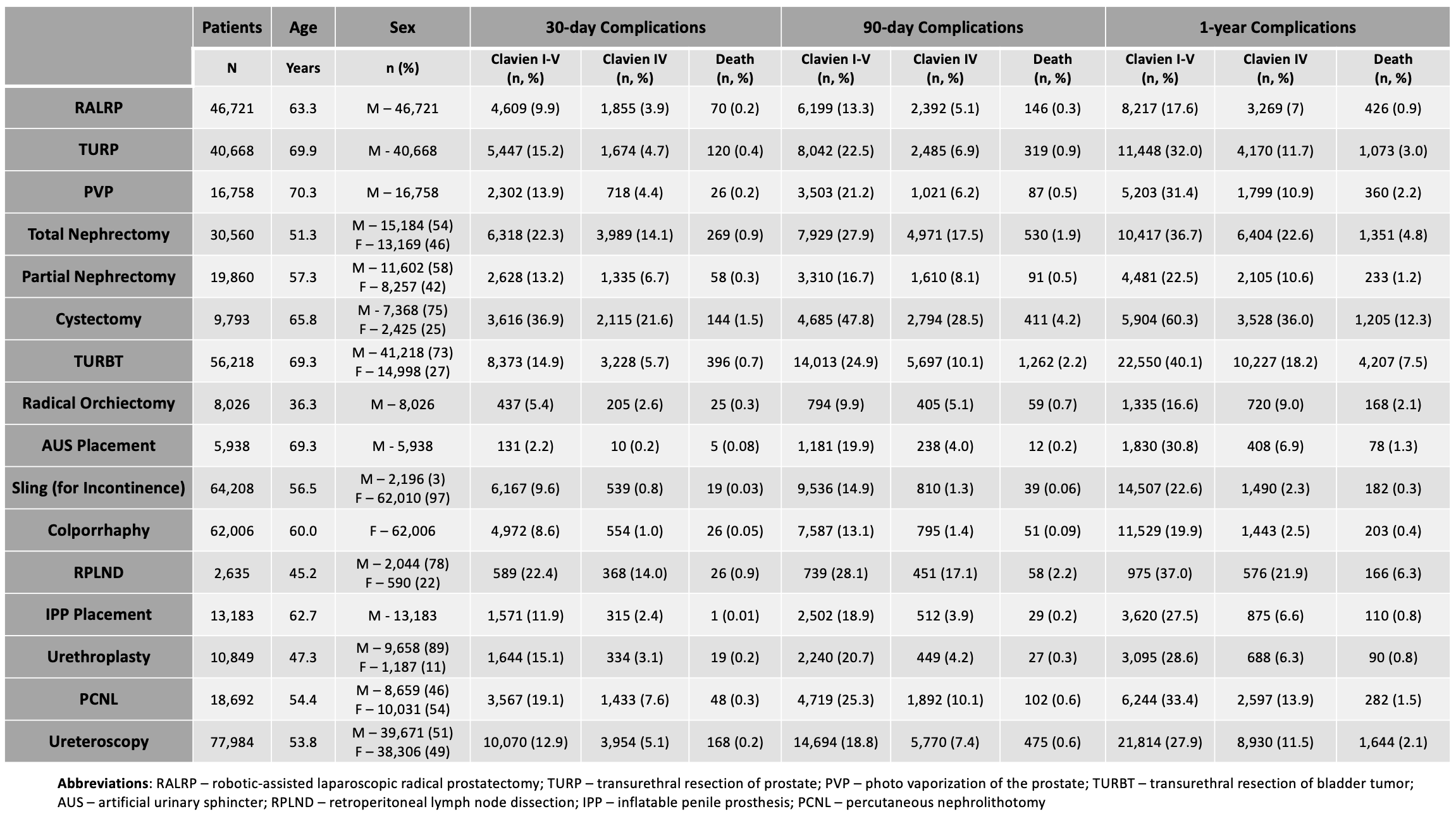
Introduction: Many studies evaluating complication rates following urologic procedures focus on a narrow subset of procedures, include the experience of select, high volume surgeons, or have variable follow-up. We systematically compare national complication rates following an array of urologic surgeries by numerous providers, which can serve as an important benchmarking tool in the pursuit of quality care. Methods: We performed a retrospective cohort study using the TriNetX research network from 2006-2022, which includes claims data for 110 million patients. Procedure type, age at index procedure, sex, race, and complications were queried using applicable CPT and ICD10 codes. Rates of all-cause (Clavien I-V), life-threatening (Clavien IV), and mortality (Clavien V) complications were evaluated using 30-day, 90-day, and 1-year timepoints from the index operation. Clavien IV complications included: sepsis, acute renal failure requiring dialysis, PE, reintubation, myocardial infarction, cardiac arrest, and re-operation. Results: A total of 484,099 urologic procedures were included. Age, sex, race, and 30-day, 90-day, and 1-year complication rates stratified by procedure are listed in Table 1. All-cause complication rates ranged from 2-37%, 10-48%, and 17-60% for 30-day, 90-day, and 1-year time points, respectively. Rates of Clavien IV complications were less than or equal to 10% at all timepoints for most procedures with notable exceptions being total nephrectomy (14-23%), cystectomy (22-36%), and RPLND (14-22%). The 1-year mortality rate for most procedures was low. Exceptions include cystectomy (12%), TURBT (8%), RPLND (6%), and total nephrectomy (5%). Procedures with the lowest rates of 30-day, 90-day, and 1-year complications included those within reconstructive urology including AUS placement, sling procedures for incontinence, colporrhaphy, IPP placement and urethroplasty. 30-day, 90-day, and 1-year mortality rates following these procedures mirrored that of the general population not undergoing surgery. Conclusions: This analysis establishes benchmark complication rates up to 1-year post-op for many urologic procedures using a national database, which can aid hospital systems in identifying deficiencies in quality care. SOURCE OF Funding: NA