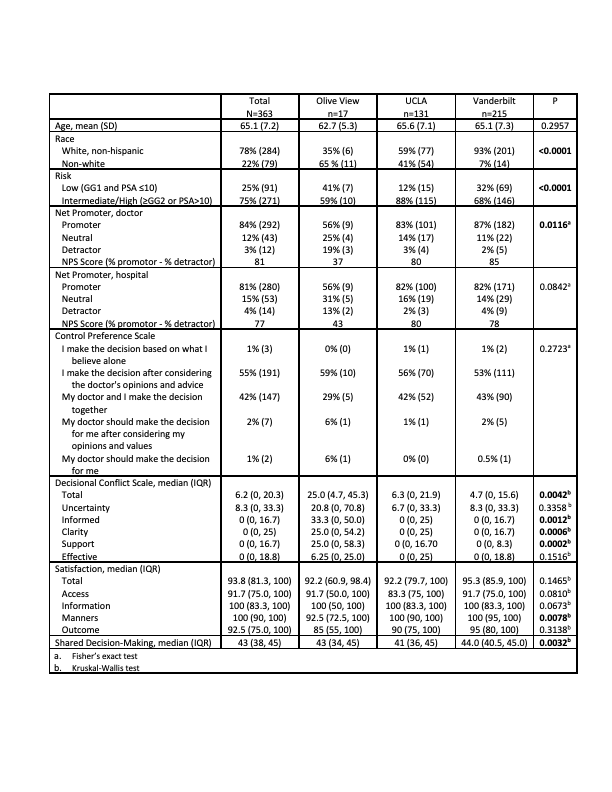
Introduction: Shared decision making (SDM) is recommended for men with prostate cancer. Implementation of SDM has proved challenging. We aimed to use the tools of implementation science to identify factors key to implementation of a successful SDM program at one institution to two new institutions with differing patient populations, including in the safety net. We also measured comparative effectiveness of the decision aid across populations. Methods: As part of the Consolidated Framework for Implementation, we used the MUSIQ tool to assess readiness for implementation at UCLA, Vanderbilt, and Olive View-UCLA (OVMC), a large safety-net institution. We used MUSIQ scores to guide pre-implementation changes at each site. We then implemented the SDM program at new sites. The program featured a decision aid (DA) which quantified individual preferences for competing treatment outcomes, and used decision analysis to provide patients and physicians with a rank ordered list of evidence-based treatments. Statistical Control Process charts were used to track implementation outcomes and guide the need for interventions to improve outcomes. Decision quality outcomes were collected using a post-consult survey. We evaluated implementation outcomes and differences in decision quality among men at the different sites. Results: MUSIQ scores were high (144, 157, and 117 out of 168 at OVMC, UCLA, and Vanderbilt, respectively), and guided pre-implementation efforts at each site. Modifications were made at each site to facilitate implementation, such as delivery of the DA in the waiting room at OVMC. Implementation outcomes were strong and preserved from the original site. Adoption among physicians was 100%. Penetration (invitation rate) and Fidelity (completion rate) were similar in academic and safety net settings (66% vs 60%, p=0.4 and 77% vs 80%, p=0.7, respectively; N=1909). At OVMC, implementation led to lower median time spent with a physician (24 minutes after implementation vs 33 minutes before, p=0.01) and a decrease in the percentage of patients who needed more than one urology clinic visit to make a treatment decision (13% vs 46%, p<0.001). Decisional quality was excellent across all sites, with high scores for satisfaction and sense of shared decision-making; post visit decisional conflict was higher at the safety net site (Table). Conclusions: Scaling a SDM program is feasible using the tools of implementation science, leading to preserved effectiveness across a variety of patient populations. SDM programs can save clinic visit time. SOURCE OF Funding: PCORI

 photo")