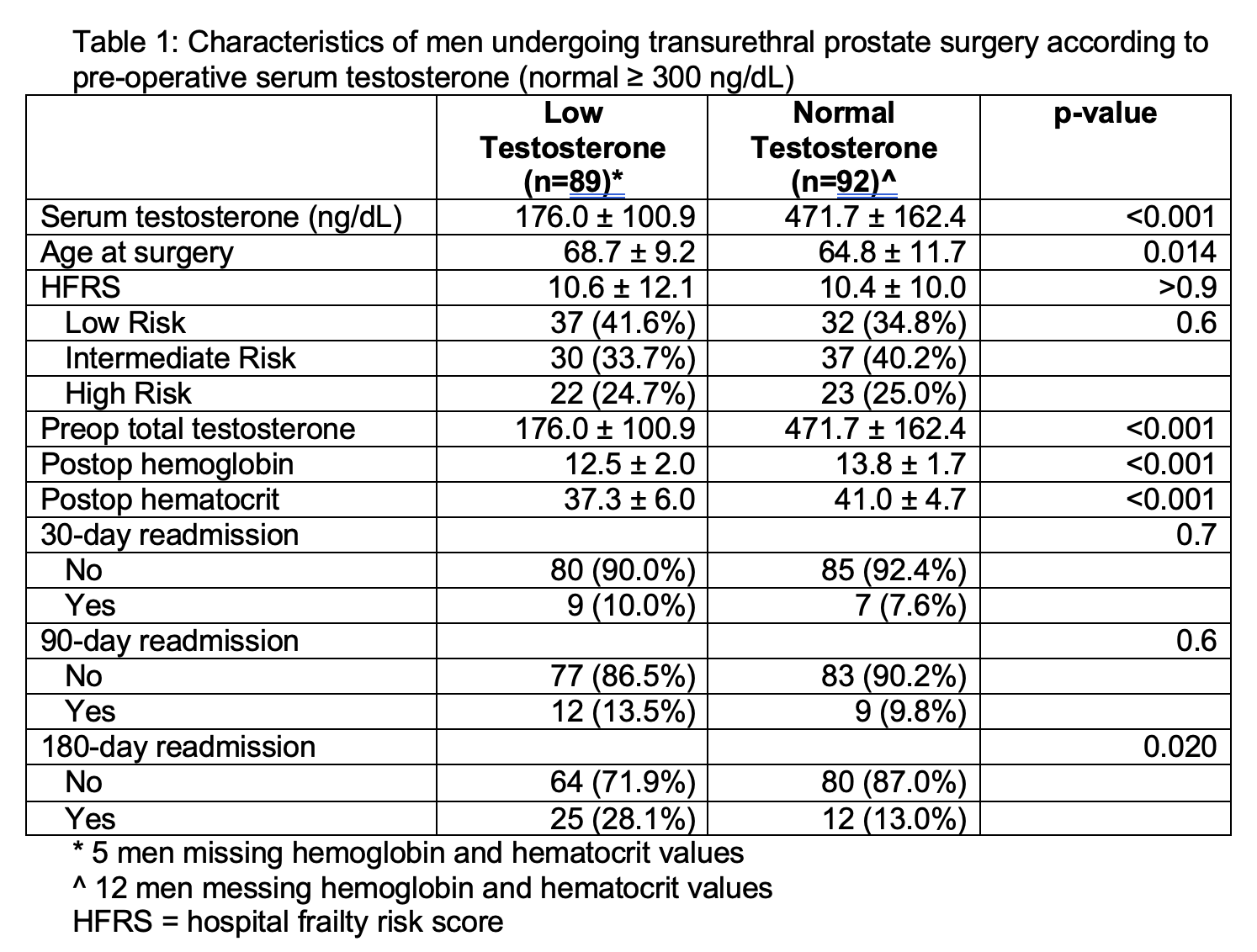
Introduction: Low testosterone (T) has been associated with decreased muscle mass, increased frailty, and a higher risk of cardiovascular disease. Therefore, low T and its consequences may adversely impact perioperative outcomes for patients undergoing surgical procedures. We sought to characterize the association between low T, frailty and perioperative outcomes in patients undergoing transurethral resection of the prostate (TURP) and laser photovaporization of the prostate (PVP). Methods: We identified men who underwent TURP or PVP with a recorded T level within 1 year prior to their procedure date. We compared the clinical characteristics, lab values, and Hospital Frailty Risk Scores (HFRS) of patients with low ( <300 ng/dL) versus normal (=300 ng/dL) T. Descriptive statistics were performed using t-test and chi-squared test, where applicable. Univariate and multivariate regression were performed to determine the association between low T and specific perioperative outcomes. Results: Among 181 patients who underwent either TURP or PVP, 89 (49%) had low T. Mean preoperative T was 176.0 (± 100.9) versus 471.7 (± 162.4) ng/dL in the low versus normal T group (p < 0.001). Patients with low T were older (68.7 ± 9.2 vs. 64.8 ± 11.7 years old, p=0.014) and had longer post-op stays (4.1 ± 10.3 vs. 1.4 ± 0.9 days, p=0.03), lower post-op hemoglobin (12.5 ± 2.0 vs. 13.8 ± 1.7, p<0.001) and hematocrit (37.3 ± 6.0 vs. 41.0 ± 4.7, p<0.001) values. Patients with low T also had higher rates of readmission within 180 days (28% vs. 13%, p=0.020). T was not independently associated with frailty (p=0.6). On multivariable analysis, both HFRS and low preoperative T were independently associated with 180-day readmission on multivariable analysis (OR 1.04, 95% CI 1.00-1.07, p=0.05 and OR 1.00, 95% CI 0.99-1.0, p=0.002, respectively). Conclusions: Almost half of men undergoing transurethral surgery had low T. While low T was not independently associated with frailty, both low T and frailty were independently associated with higher risk of 180-day readmission. While future prospective studies are needed, low T may be an independent risk factor for adverse perioperative outcomes after transurethral surgery, indicating a potential for T assessment and possibly treatment pre-operatively. SOURCE OF Funding: Urology Care Foundation Research Scholar Award SP0071384