University of Wisconsin School of Medicine and Public Health
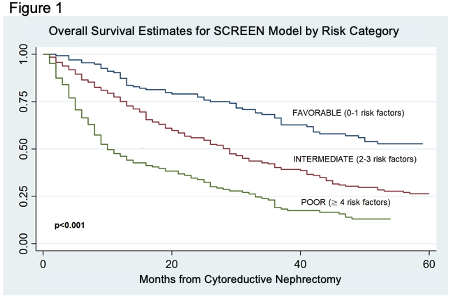
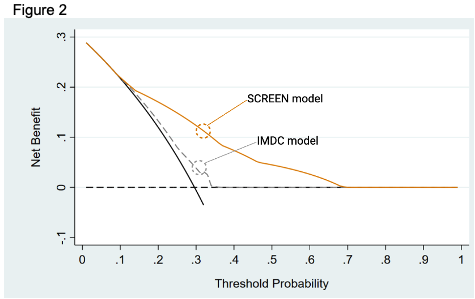
Introduction: Patient selection for cytoreductive nephrectomy (CN) is critical yet few studies incorporate tumor burden into decision making. This study developed a prognostic model to improve CN selection by integrating radiologic features with known prognostic factors. Methods: Consecutive mRCC patients treated with upfront CN at 5 institutions from 2006-2017 were included. Preoperative axial imaging was analyzed for measures of tumor burden including number of sites, total metastatic tumor burden (sum of metastatic lesions’ maximum diameter) and maximum primary tumor diameter. Univariable/multivariable Cox models were used to evaluate known prognostic variables associations with overall survival, and the SCREEN model was constructed using independently predictive preoperative variables. This model was compared to the IMDC model for predictive accuracy and clinical utility. Results: A total of 914 mRCC patients were treated with upfront CN during the study period. Seven independently predictive variables used in the SCREEN score included: number of metastatic sites = 3, total cm of metastatic tumor burden = 5 cm, bone metastasis, systemic symptoms, low serum hemoglobin, low serum albumin, and neutrophil to lymphocyte ratio = 4. Risk groups were created based on number of risk factors (Figure 1). The SCREEN model demonstrated improved survival discrimination compared to the IMDC risk groups. When evaluating early mortality (death =12 months from CN), predictive accuracy measured by the area under the ROC curve was 0.76 for SCREEN compared to 0.55 for the IMDC model. Decision curve analysis showed that the SCREEN model improved decision making beyond IMDC score for threshold probabilities of early mortality between 15-70% (Figure 2). Conclusions: The SCREEN model integrates radiographic measurements for mRCC patients, which was associated with improved predictive accuracy. These findings should be validated further in independent cohorts. SOURCE OF Funding: None

.jpg "Daniel Shapiro, MD (he/him/his) photo")