MP56-03: A Complimentary Analysis of Plasmacytoid Urothelial Carcinoma of the Bladder: Genomic Landscape Independent of Somatic CDH1 Mutations and Real-World Clinical Outcome Study
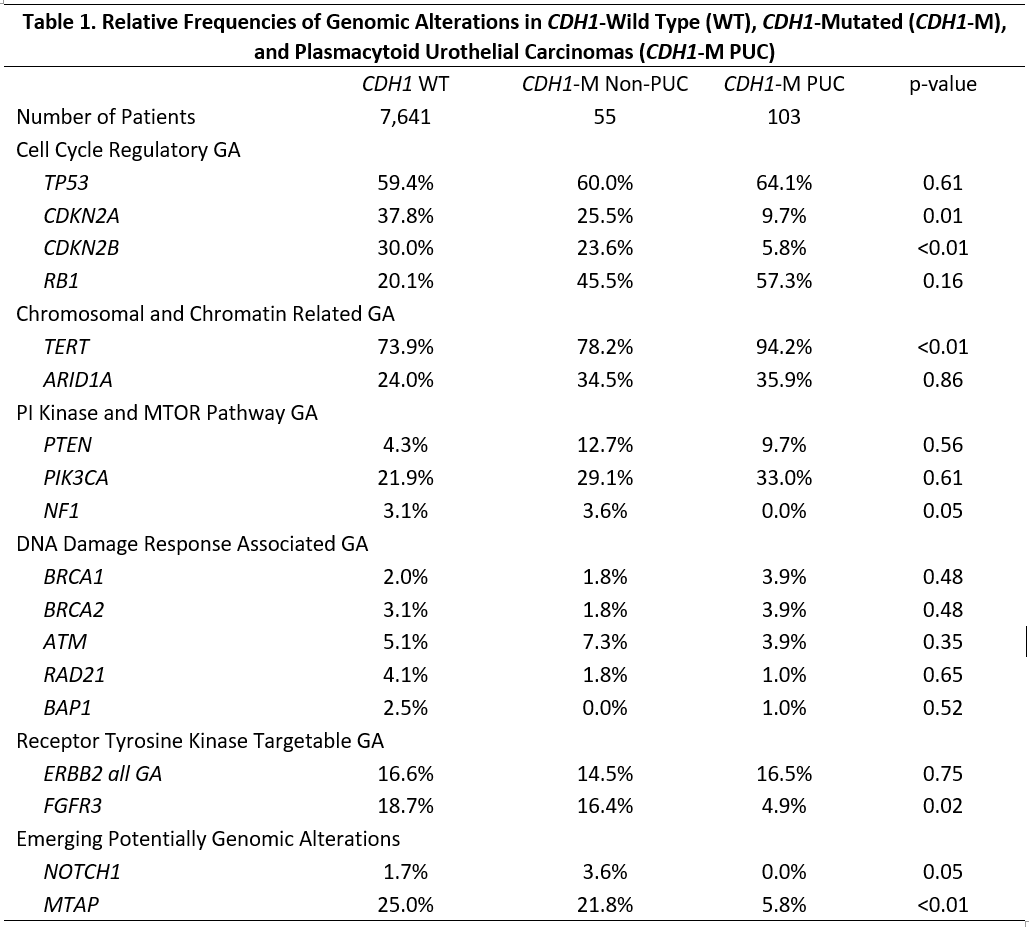
Introduction: Plasmacytoid urothelial carcinomas of the bladder (PUC) represent an aggressive malignancy with somatic CDH1 mutations, poor survival, and few systemic therapy options. We aimed to analyze the genomic landscape of urothelial carcinomas stratified by CDH1 status and PUC histology, while utilizing real-world clinical outcome data. Methods: 7,903 clinically advanced patients with UCB underwent hybrid capture based comprehensive genomic profiling (CGP) to evaluate all classes of genomic alterations (GAs) as well as microsatellite instability (MSI), tumor mutational burden (TMB), and genomic loss of heterozygosity (gLOH, high =16%). Plasmacytoid histology was confirmed by pathologic evaluation. GAs were compared by plasmacytoid histology and CDH1-mutated (CDH1-M) vs. wild-type (WT). The Flatiron Heath-Foundation Medicine Urothelial Clinico-Genomic Database (FH-FMI CGDB) was used to characterize overall survival (OS) and progression-free survival (PFS) in CDH1-M vs. WT, stratified by systemic therapy administered. Results: CDH1 mutations were identified in 158 patients, who demonstrated a higher frequency MSI-high status (2.7% vs. 0.8%, p<0.01), mean TMB (14.8 vs. 9.9%, p<0.01), but lower gLOH (6.8% vs. 20.3%, p<0.01). PUC was identified on pathologic analysis in 103 (65%) patients with CDH1 mutations. Table 1 demonstrates the frequency of GAs between these three groups. There were no differences in genes associated with DNA damage response. In the non-PUC cohort, GAs on chromosome 9p21 were increasingly mutated. From the FH-FMI CGDB, 22 patients (3.7%) featured CDH1 mutations, and shared similar demographics to CDH1-WT. These patients demonstrated worse OS (OS 3.3 vs. 9.5 months, p=0.03) and PFS (2.8 vs 3.5 months; p=0.09) when treated with immune checkpoint inhibitors, but no difference following chemotherapy. Conclusions: CDH1 mutations are not exclusive to PUC, which possesses a distinct genomic profile and natural history. Real-world clinical outcomes support that CDH1 mutations predict resistance to immune checkpoint inhibition, but not chemotherapy. Taken together, these results further support genomic profiling of advanced bladder tumors and treatment individualization based on genomic signatures. SOURCE OF Funding: NA