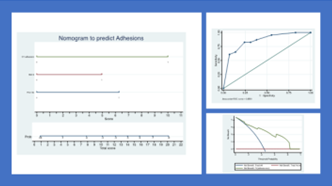
Introduction: Intraabdominal adhesions are nonspecific complications related to prior abdominal surgery. Aim of our study was to evaluate the possible preoperative predictors of abdominal adhesions. Methods: A consecutive series of patients undergoing abdominal surgery were prospectively enrolled from January 2021 to October 2022. Patients were preoperatively evaluated with clinical history and physical examination. A contrast enhanced CT scan was performed before the procedure and on the portal phase intrabdominal adhesions were recorded. Intraoperative adhesions were graded according to the peritoneal carcinomatosis index. Predictors of intraoperative adhesions were evaluated using logistic regression analysis. A nomogram was developed based on the logistic regression model. Results: Overall, 104 patients with a median age of 69 (64/73) were enrolled. On abdominal CT 58/104 ( 56%) presented signs of abdominal adhesions and 46/104 (44%) presented adhesions intraoperatively. Median PCI was 5 (3/7). Patients with intraoperative abdominal adhesions presented more frequently Metabolic Syndrome ( 37/46: 82% vs 30/58: 51%, p<0,05), previous abdominal surgery ( 32/46:69% vs 21/58: 37%, p<0,01), ischemic heart disease (IHD) ( 16/46:36 % vs 9/58: 16 %, p<0,05) and signs of adhesions on abdominal CT ( 40/46: 87% vs 18/58:31%; p<0,05). On univariate analysis, metabolic syndrome, IHD, prior abdominal surgery and CT adhesions were predictors of intraoperative adhesions. On multivariate analysis, metabolic syndrome, abdominal surgery and CT adhesions were predictors of intraoperative adhesions. We developed a clinical nomogram to predict adhesions with an AUC of 0,85 and a clinical net benefit in the range of probabilities between 20 and 80%. Conclusions: Metabolic syndrome, prior abdominal surgery and CT adhesions are predictors of intraoperative adhesions. The present nomogram may be used after external validation to counsel patients on the presence of adhesions before abdominal surgery. SOURCE OF Funding: None

 photo")