Session: MP28: Kidney Cancer: Advanced (including Drug Therapy) I
MP28-06: Clinical implications and predictive factors of primary resistance to nivolumab plus ipilimumab therapy in patients with metastatic renal cell carcinoma
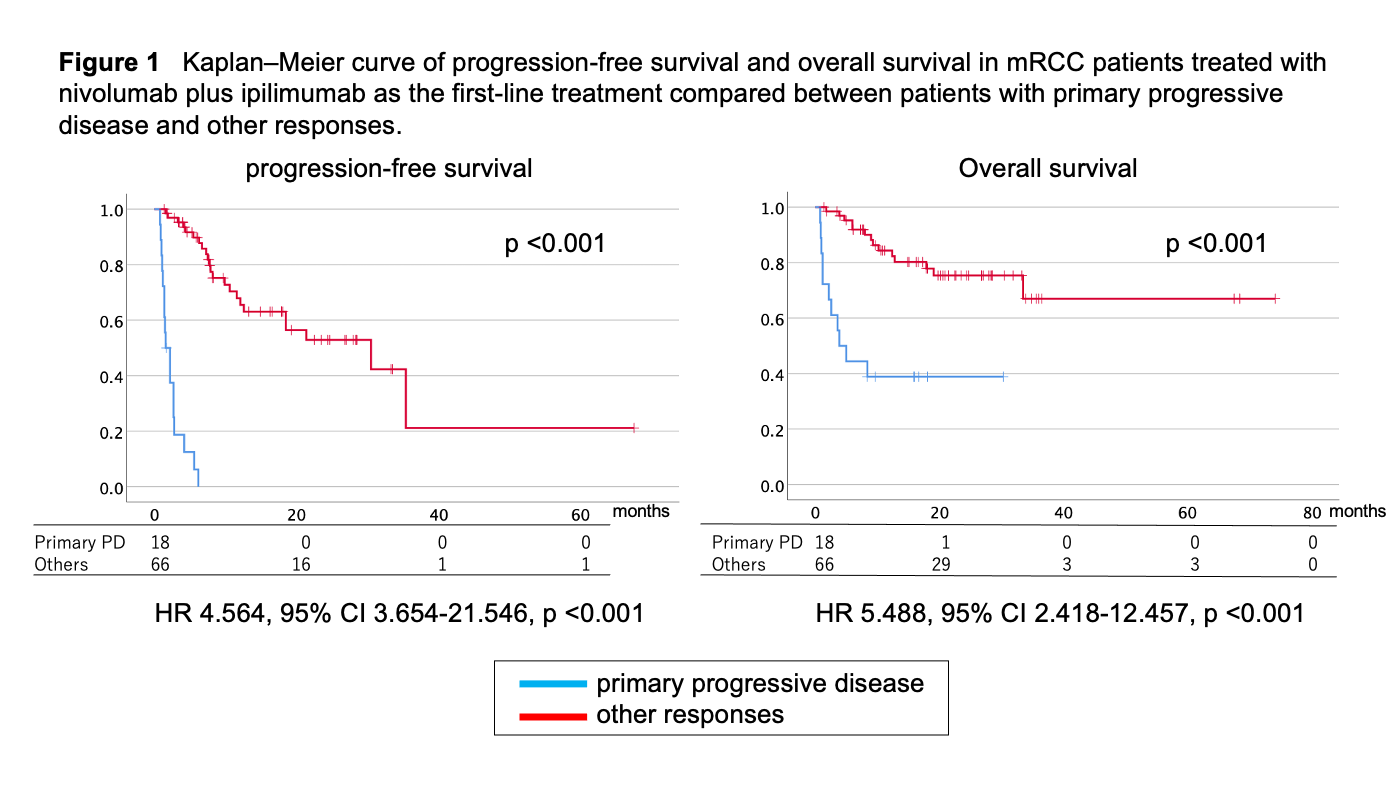
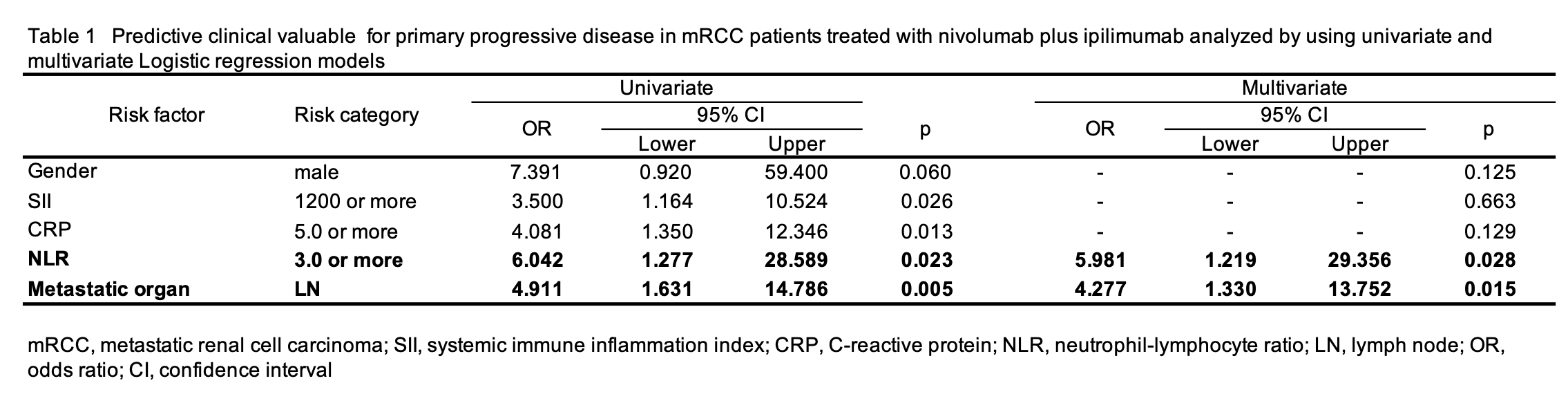
Introduction: Nivolumab plus ipilimumab (NIVO+IPI) is the established first-line treatment for patients with metastatic renal cell carcinoma (mRCC). Although median overall survival (OS) of mRCC expects nearly four years, almost 20% of patients showed primary resistance to NIVO+IPI. To know whom patients do not expect any benefit from NIVO+IPI must gather attention from clinicians. These patients might be better given other immune-oncological (IO) combination regimens to avoid wasting limited lifetime and unnecessary immune-related adverse events. We aimed to evaluate the risk factors of primary resistance to NIVO+IPI in patients with mRCC. Methods: We retrospectively evaluated 89 patients with mRCC treated with NIVO+IPI from multiple institutes. Primary resistance was defined as a progressive disease diagnosed by the first imaging evaluation. The associations between clinical factors and primary progression disease (pPD) were analyzed. Results: The median observation period was 15.1 months (1 to 74 months). A total of 18 pPD occurred (20%) after NIVO+IPI initiation. Patients experienced pPD showed extremely worse overall survival (hazard ratio 5.488, 95% confidence interval [CI] 2.418-12.457, p <0.001) (Figure 1). The univariate analysis resulted that male gender, high systemic immune inflammation index, high C-reactive protein, high neutrophil-lymphocyte ratio (NLR), and metastasis in lymph node (LN) were related to pPD. In multivariable analysis, the LN metastasis (odds ratio [OR] 4.277, 95%CI 1.330-13.752, p = 0.015) and NLR > 3 (OR 5.981, 95%CI 1.219-29.356, p = 0.028) were an independent risk factor of pPD (Table 1). All pPD patients had at least one risk or both. Conclusions: This retrospective study showed that LN metastasis and high NLR were associated with pPD independently in patients treated with NIVO+IPI as first-line therapy. These patients might better be treated with other IO combinations such as VEGFR-TKI+IO. SOURCE OF Funding: None