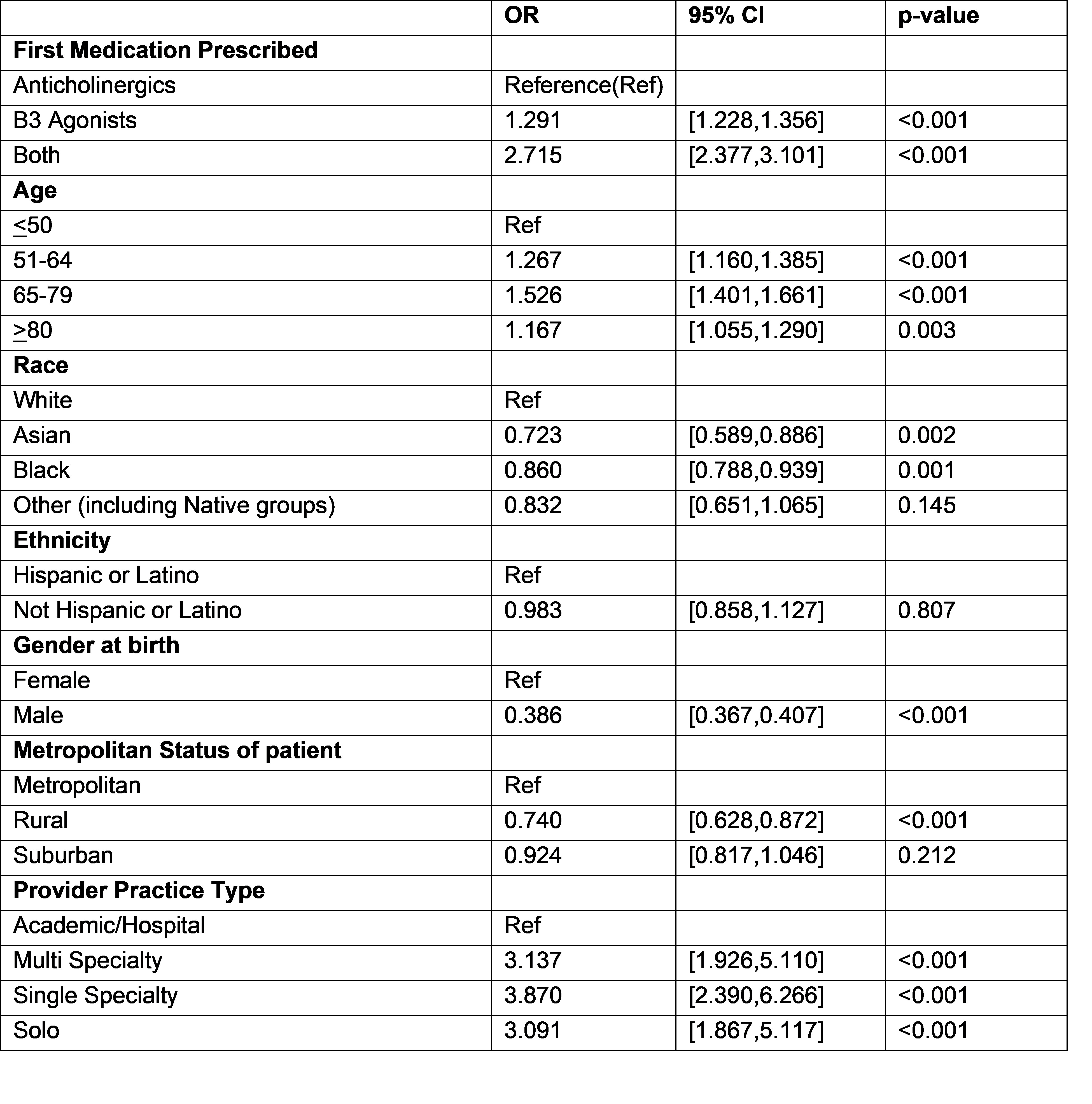
Introduction: Third line therapies for Overactive Bladder (OAB) include Percutaneous Tibial Nerve Stimulation (PTNS), Sacral Neuromodulation (SNS) and OnabotulinumtoxinA bladder injections (BTX-A). The American Urologic Association (AUA) and Society for Urodynamics, Female Pelvic Medicine and Reconstructive Surgery (SUFU) have jointly developed a guideline to help manage patients with OAB. Using the AUA Quality (AQUA) registry, we aim to assess access and implementation of third line therapies. Methods: The AQUA registry collects data from participating urologists across practice settings by direct interface with local electronic health record systems. We queried the registry for patients >18 years with a new diagnosis of OAB, urinary urgency, frequency, and urgency urinary incontinence (UUI) from 2014-2020 using ICD9 and ICD10 codes with >1 year follow up. We evaluated patients who proceeded to third line therapy by insurance type, gender, ethnicity, metropolitan status, age and medication type. We excluded patients with a diagnosis of neurogenic bladder. Multivariable regression was performed to determine the odds ratio of progression to third line therapy. Only patients who first received second line therapy prior to third line therapy were included in the analysis. Results: A total of 1,401,168 patients were diagnosed with OAB during the study period. Complete data was available for 641,122 and analysis was performed specifically for this cohort. 112,021 (17.5%) patients received second line therapy with either an anticholinergic, beta-3 agonist or combination therapy. Of those, 7,487 (1.2%) received at least one third line therapy. BTX-A was the most common therapy overall (40%, 32% SNS, 28% PTNS), while PTNS was the most common third line therapy in men (35%), Asian patients (37%), patients aged > 80 (40%) and patients seen in solo practitioner (46%) settings. Black and Asian race, male gender and rural setting had lower odds of progressing to third line therapy. Patients seen by providers in multi-specialty settings, single specialty settings and solo practices were approximately 3 times more likely to receive third line therapy than in an academic medical center (Table 1). Conclusions: In this study, a small percentage of patients progress from second to third line therapy. Rates varied amongst gender, race, metropolitan status and practice setting. These findings highlight opportunities to improve third line therapy implementation. SOURCE OF Funding: AUA Data Committee