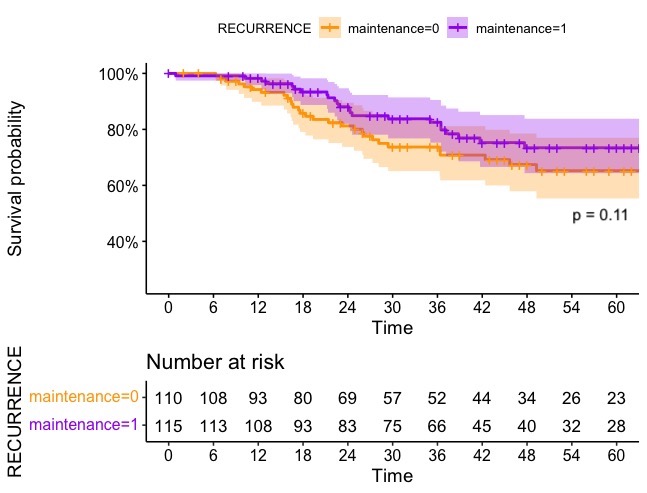
Introduction: The use of repeated Mitomycin C (MMC) instillation in low- (LR) and intermediate-risk (IR) Non-Muscle Invasive Bladder Cancer (NMIBC) is still a matter of discussion among the urological community. The aim of the current study was to analyze long term outcomes of maintenance regimen of repeated MMC instillations in LR and IR patients. Methods: We identified 228 patients diagnosed with NMBIC after transurethral resection of bladder tumor (TURBT) that underwent MMC instillations between 2013 and 2022 at a tertiary referral center. All patients felt within the criteria for LR or IR class according to European Association of Urology Guidelines. Recurrence-free survival (RFS) was analyzed and compared with Cox-derived univariate Kaplan-Meier (KM). A Multivariable Cox-regression analyses (MVA) assessed the impact of MMC maintenance regimen on RFS (covariates: T stage, grade, multifocality, early instillation). Subgroup analysis evaluated the effect of MMC instillations number on RFS in patients who received maintenance. Results: Overall, 89 (39%) and 139 (61%) patients were diagnosed with LR and IR NMIBC, respectively. Low grade lesions were found in 88% (n=200) of cases. Pathological Ta tumors were 93% (n=211) and multifocality was present in 107 cases (47%). Median age at diagnosis and follow-up time were 71 (IQR 62-77) and 44 months (IQR 28-63), respectively. Early instillation was performed in only 21 patients (9.2%). Recurrence occurred in 57 patients (25%). All patients underwent MMC induction with 89% rate of 6-instillations cycle completion; 118 patients (51%) underwent maintenance instillations with a median number of instillations equal to 9.5 (6-11). Overall, RFS at 5 years follow-up was 69.6% [62.7, 77.2]. Patients who did or did not receive MMC maintenance had a 5-years RFS of 73.4% vs 65.2%. At MVA, MMC maintenance and number of instillations did not significantly correlate with a better RFS. Conclusions: Our study showed that MMC maintenance instillations do not reduce the risk of recurrence in LR and IR NIMBC patients who received MMC induction. SOURCE OF Funding: None

 photo")