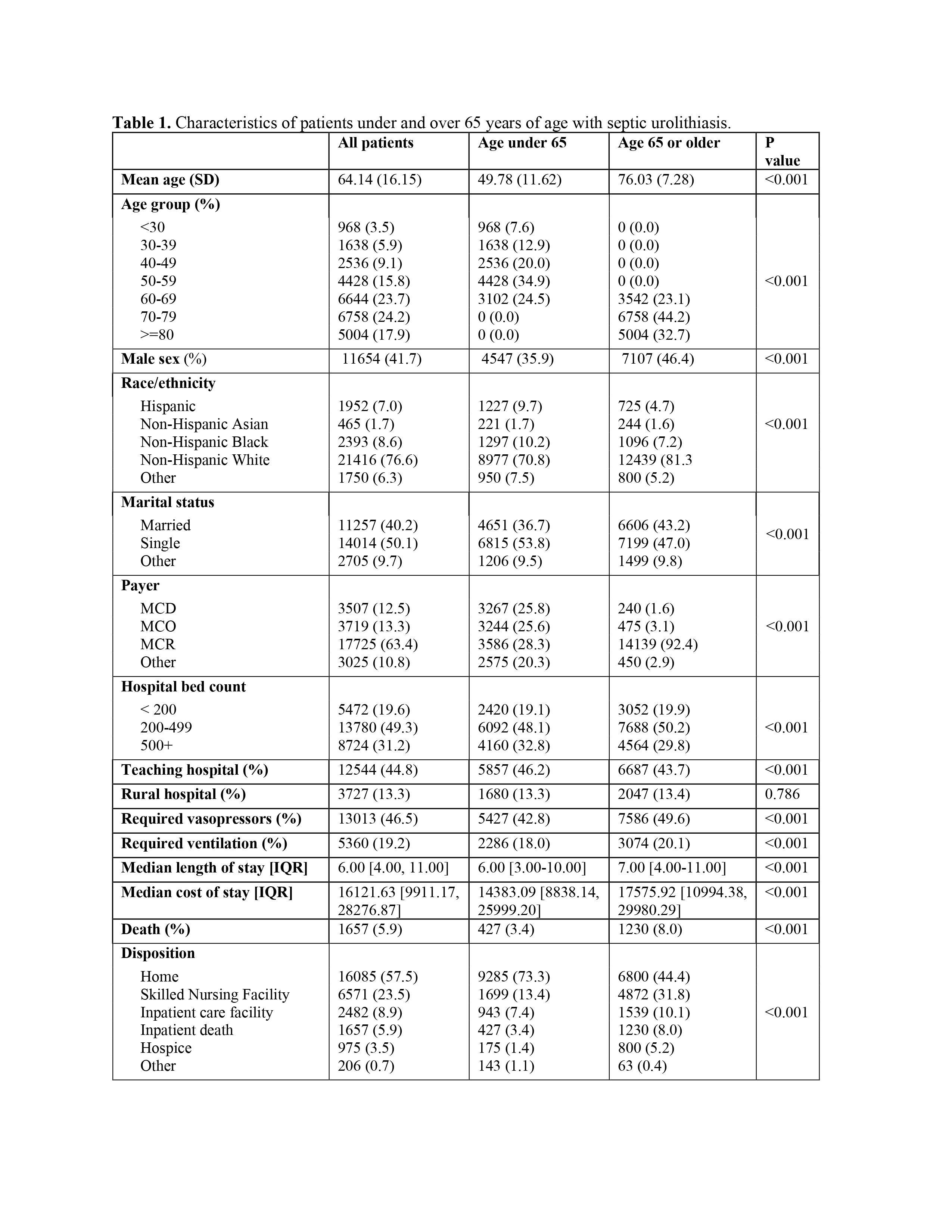
Introduction: An obstructing urinary tract stone complicated by infection (septic stone) requires urgent intervention with both antibiotics and urinary tract decompression. Delayed treatment can lead to significant morbidity and sometimes mortality. Current published claims analyses reflect data up to 2011. Given a rapidly aging population and advances in critical care, we sought to examine characteristics and outcomes of patients with sepsis secondary to obstructing stones in a contemporary cohort, with a focus on outcomes in older adults. Methods: We conducted a retrospective cohort study using data from the nationwide Premier Healthcare claims database (2016-2020) to identify hospital inpatients aged 18-95 treated for septic urolithiasis, using ICD-10 diagnostic codes consistent with sepsis with urinary stones. Baseline sociodemographic factors were described and stratified into 2 age groups: adults 65 years and older defined as “older adults”, and adults aged <65 years defined as the “younger cohort”. Outcomes such as length of stay, mortality, and discharge disposition were also compared in the 2 groups. Results: The study cohort included 27,976 patients, of which 15,304 (54.7%) were older adults (Table 1). The average age of older adults was 76.0 (SD ±11.6) years, compared with 49.8 (SD ±7.3) years in younger cohort (p < 0.001). Among older adults, 46.4% were male, versus 35.9% in the younger cohort; overall the cohort was predominantly non-Hispanic white (76.6%). Older adults were less likely to be cared for in teaching hospitals (p < 0.001), and more likely to be cared for in smaller hospitals ( <500 beds, p<0.001). Despite receiving more aggressive care (invasive mechanical ventilation, vasopressor use) and incurring higher costs (p < 0.001), older adults experienced substantially higher mortality (RR 2.35, 95% confidence interval 2.1-2.7, p<0.001). In addition, older adults were significantly more likely to be discharged to a skilled nursing facility (31.8%) than younger adults (13.4%). Conclusions: Older adults hospitalized with septic stones have significantly worse outcomes, receive more aggressive care, and incur higher healthcare costs. Additional investigation is needed to identify patient, clinician, and facility-level drivers of these outcomes, so as to create pathways to reduce disparities and optimize outcomes for older adults. SOURCE OF Funding: Duke University

 photo")