MP18-18: What If They Continued The Pregnancy? Using Prenatal Ultrasound Findings to Predict Postnatal Outcomes for Fetuses with Lower Urinary Tract Obstruction (LUTO) To Improve Counseling and Aid in Decision Making
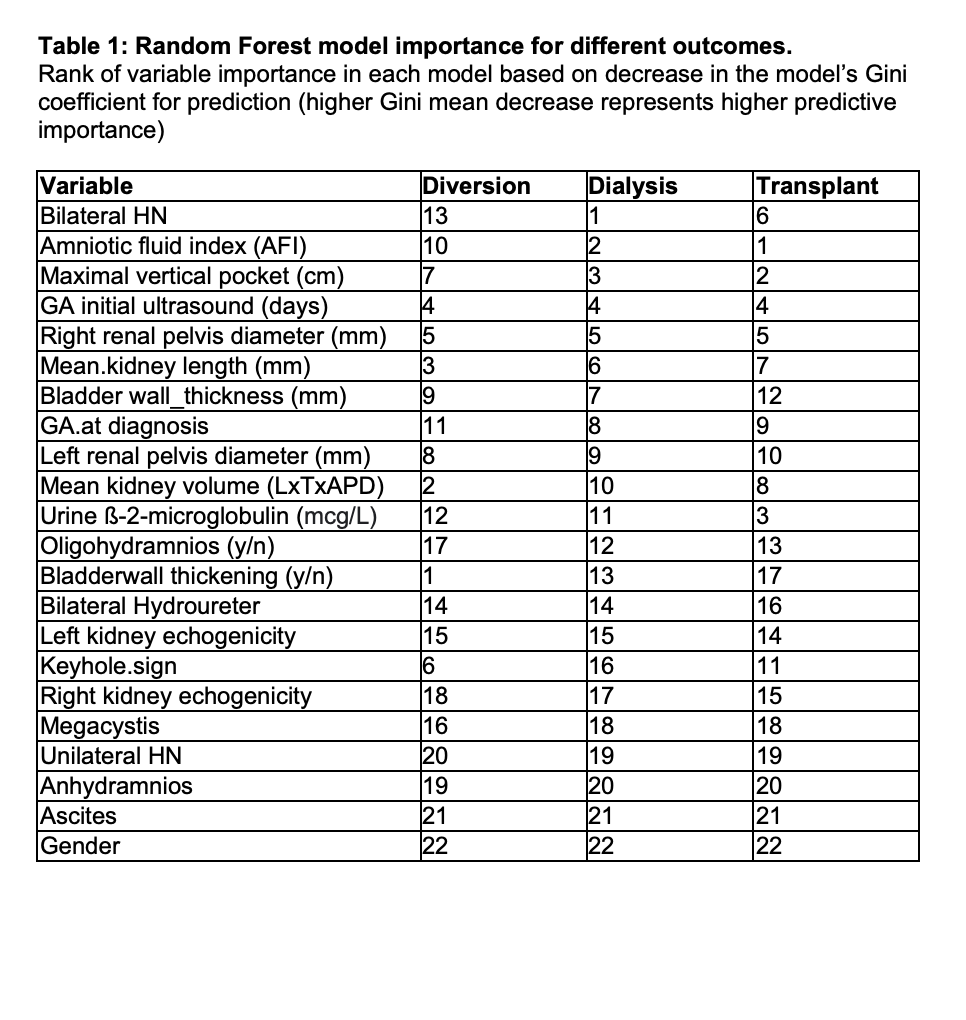
Introduction: LUTO is a chronic condition with a spectrum of outcomes. It is usually suspected prenatally based on ultrasound features (USF). Given the unknown postnatal trajectory and the potential for significant morbidity and mortality, many families choose termination of pregnancy (TOP), often based on USF alone. We sought to develop a tool that can be used to predict postnatal outcomes based on combinations of USF to aid with prenatal counselling and parental decision making. Methods: We reviewed a LUTO database from a high-risk fetal center and tertiary pediatric center and collected USF and postnatal need for urinary diversion and renal replacement therapy (RRT). USFs from a gestational age (GA) of 13-26 weeks for TOPs were collected and matched to fetuses who were not terminated to build a random forest model. Each predictor was assessed independently with combined importance when accounting for other predictors (see Table 1). The model was used to predict the most likely postnatal outcomes for TOPs had the pregnancy been continued. Results: USF from 37 TOPs and 30 livebirths with postnatally confirmed LUTO were included with a follow up time of 1599 days. There were 4 postnatal deaths. Dialysis was predicted with the highest accuracy of 81% (63% sensitivity, 89% specificity), with transplant second highest (69%, 43% sensitivity, 79% specificity), and diversion the least well predicted (50% accuracy). For TOPs, had the pregnancies continued, the model predicted dialysis in 16/37 (43%), transplant in 7/37 (19%) cases, and urinary diversion in 17/37 (46%). All TOPs predicted to receive transplant were predicted to receive diversion and/or dialysis, with the majority receiving both (5/7). This is similar to the postnatal LUTO cases in which 6/7 transplanted cases received both diversion and dialysis. Conclusions: Our data suggests that it is possible to predict postnatal renal replacement therapy from USFs in TOPs had the pregnancy been continued. Predictive accuracy will improve with continued follow-up of more patients, enabling more personalized prenatal counseling and allowing for more informed decision making for families. SOURCE OF Funding: None

 photo")