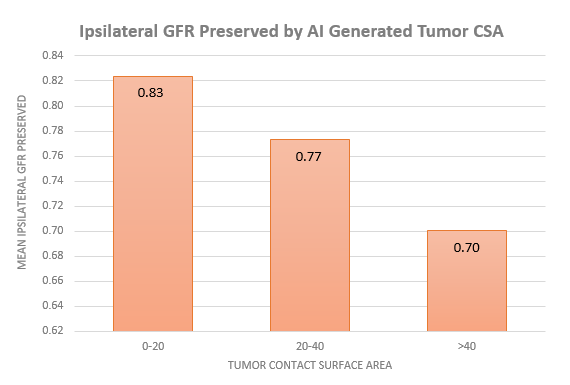
Introduction: Tumor Contact Surface Area (CSA) is an externally validated nephrometry scoring system that requires measurement of multiple dimensions of cross sectional imaging. Despite studies demonstrating its ability to predict glomerular filtration rate (GFR) following partial nephrectomy (PN), its implementation has been slowed by required time investment and interobserver variability. We sought to evaluate the utility of artificial intelligence (AI) generated CSA as compared to human-generated CSA in predicting post-PN GFR. Methods: A total of 300 patients with preoperative computerized tomography with early arterial contrast phase were identified from a cohort of 544 consecutive patients undergoing surgical extirpation for suspected renal cancer. A deep neural network approach was used to automatically segment kidneys and tumors, and then programed to generate the measurements and calculate tumor CSA. Human CSA scores were independently calculated by medical personnel blinded to AI-scores. Ipsilateral GFR before and after surgery was calculated from volumetric analyses of kidney parenchyma and pre and post-operative GFR values. AI-CSA and Human-CSA were then compared with regards to their ability to predict Ipsilateral GFR preservation. Results: After removal of patients undergoing RN and those without requisite data for GFR calculation, a total of 150 patients were included in the analysis. There was significant agreement between Human CSA and AI-CSA on linear regression analysis (R2 = 0.74, p <0.0001). On univariate linear regression analysis, both AI- (r=0.217, p =0.0076) and Human generated (r=0.187, p=0.021) CSA similarly predicted ipsilateral GFR preservation. However, when incorporated into a MV model incorporating age, gender, body mass index, diabetes status, and ischemia time, only AI generated tumor CSA remained a significant predictor of ipsilateral GFR preservation (p = 0.021). Conclusions: Fully automated tumor CSA calculations are not inferior, and may be superior, to human generated CSA calculations in predicting post-operative GFR after PN. Once validated, our results suggest that AI generated CSA could be delivered automatically from a preoperative CT scan to a clinician and patient at the point of care to aid in decision making. SOURCE OF Funding: None