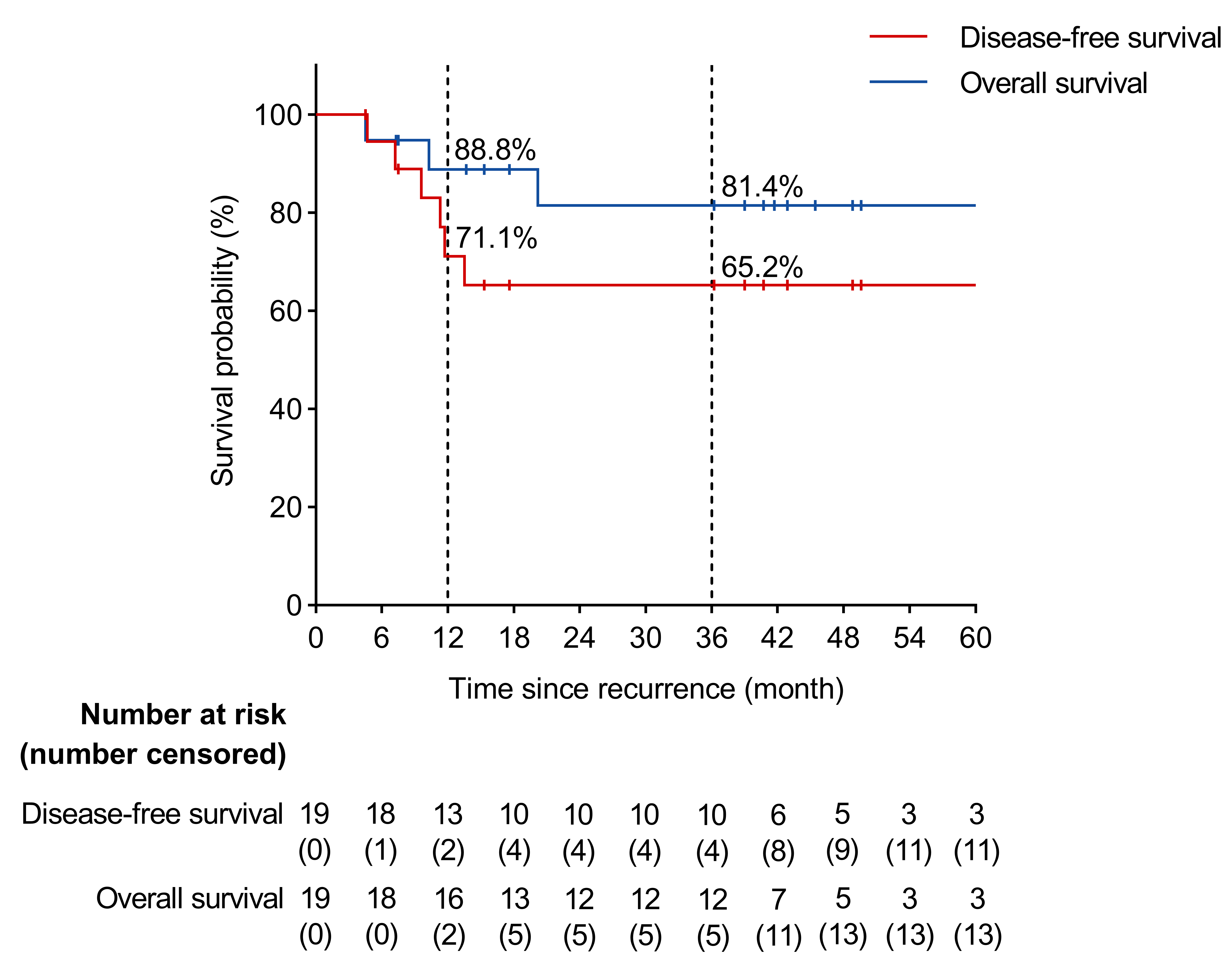
Introduction: For highly selected patients with muscle-invasive bladder cancer (MIBC), a multidisciplinary protocol of bladder-preserving therapy includes radiotherapy with concomitant chemotherapy. Some patients confer intravesical nonmuscle-invasive (NMIBC) recurrence. A retrospective study was carried out to explore the tolerability of BCG administration after chemo-radiotherapy in these patients. Methods: Patients with clinical stage T2-T4aN0M0 urothelial carcinoma of the bladder were enrolled in the analysis (some were enrolled in the clinical trial, NCT02861196). The bladder-preserving strategies were described as follows: 1) cT2 patients underwent a maximal transurethral resection (TURBT), while cT3-T4a patients underwent a biopsy; 2) All patients received neoadjuvant chemotherapy with a gemcitabine/cisplatin regimen; 3) patients then completed maximal TURBT, and those who with pT0 or downstaging to pT1/pTa received concurrent chemo-radiotherapy; 4) patients with intravesical NMIBC recurrence were recommended with TURBT followed by BCG administration. The BCG instillation schedules were as follows: 1) the induction therapy- BCG 120mg weekly for 6 cycles; 2) a 3 mo gap; 3) the maintenance therapy- BCG 120mg weekly for 3 cycles; 4) repeat the maintenance therapy every 6 mo for 1 yr to 3 yr. Results: Between 2012 and 2021, 19 patients with NMIBC recurrence underwent BCG administration after bladder-preserving therapy. All patients completed the BCG induction therapy, and 11 of 19 (57.9%) patients started maintenance therapy. Median follow-up since the recurrence was 36.2 mo. The 1 yr/3 yr probabilities of disease-free survival (DFS) and overall survival (OS) were 71.1%/65.2% and 88.8%/81.4% respectively. The most frequent BCG-related adverse events were bladder irritation (17/19, 89.5%), followed by hematuria (3/19, 15.8%), fever (1/19,5.3%), arthritis (1/19,5.3%), and bladder tuberculosis (1/19,5.3%). None of them had bladder contracture post BCG instillation. Conclusions: In summary, the tolerability and efficacy of BCG instillation after chemo-radiotherapy in NMIBC recurrence are acceptable and controllable. This study provides an alternative strategy rather than radical cystectomy in the comprehensive bladder-preserving therapy for MIBC. SOURCE OF Funding: None.

 photo")