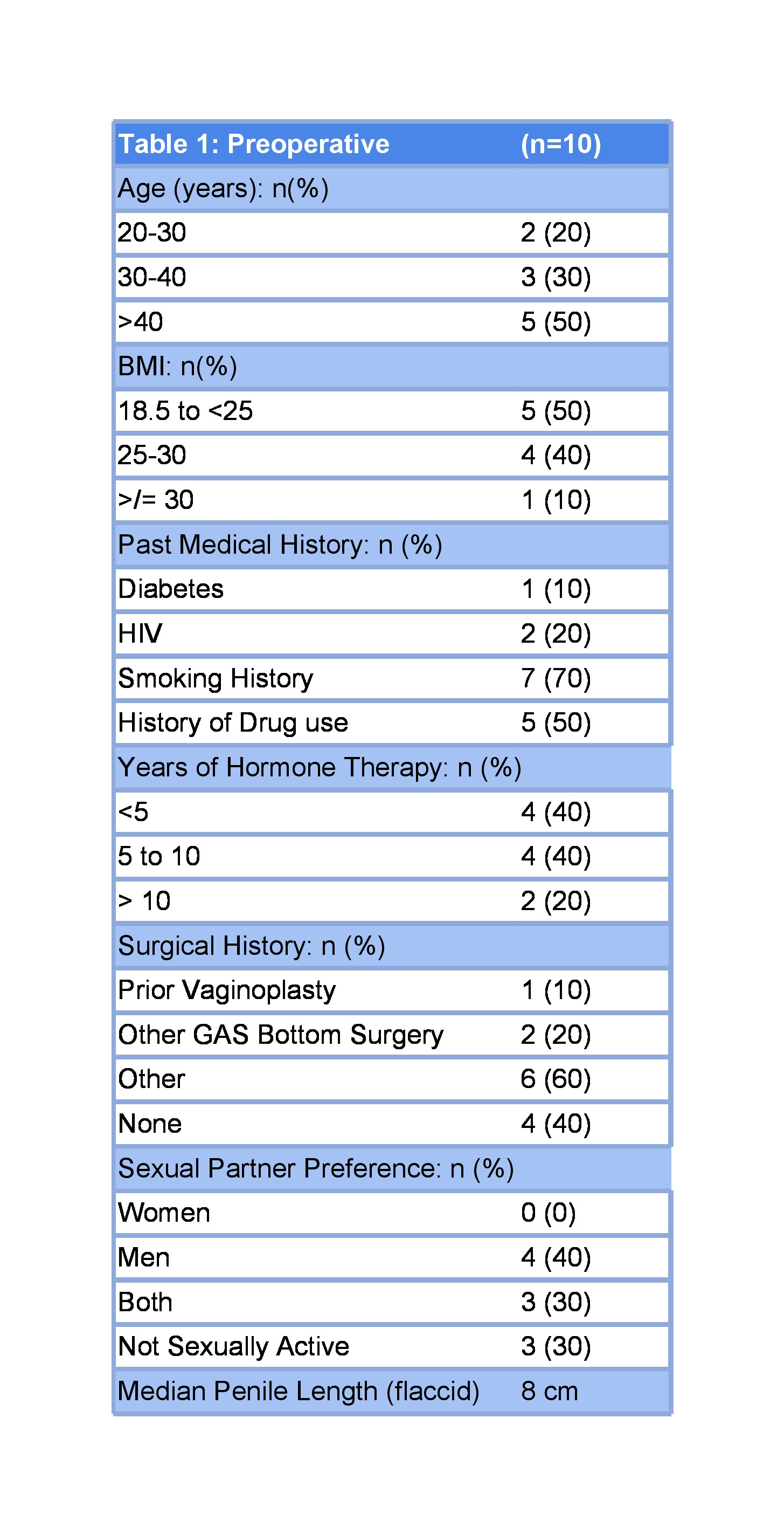
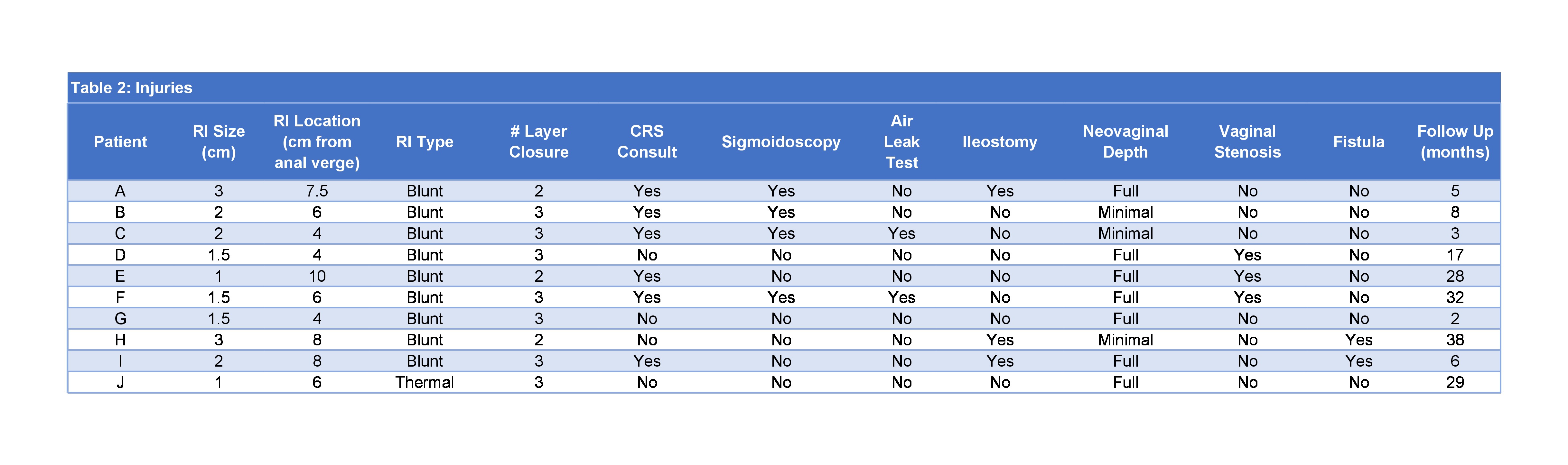
Introduction: We describe incidence, management and outcomes of rectal injuries (RI) during gender affirming vaginoplasty (GAV) and revision vaginoplasty (RV) at a high volume center. Methods: All intra-operative RI during GAV and RV are reported to a quality control committee for evaluation at our institution. We performed a retrospective review of pre-operative, intra-operative and post-operative findings of all patients with RI during GAV. Results: RI occurred in 9 of 1011 (incidence 0.89%) primary GAV and during 1 RV for vaginal stenosis from January 2016-September 2022. Preoperative data are summarized in table 1, and injury and repair characteristics in table 2. Colorectal surgery (CRS) evaluation included sigmoidoscopy in 4 cases, an air leak test in 2, and with temporary bowel diversion in 3 (2 concomitant and 1 delayed). In 7/10 full depth GAV was completed; 3 were converted to minimal depth vaginoplasty. 3 cases had unusual adhesions, obliterated planes, or fibrosis from prior silicone implant surgery during the vaginal canal dissection. 2 had bulbospongiosus muscle interposition over the repair site. No patient had a concomitant urethral injury, 2 (20%) developed a rectovaginal fistula (RVF). Both RVF occurred in patients with prior perineal surgery, including prior vaginoplasty. Neither patient had intra-operative sigmoidoscopy done by CRS. 3 patients (43%) with full depth GAV developed vaginal stenosis postoperatively. Conclusions: Rectal injuries occur even in experienced hands with an incidence of <1% in our series of 1011 patients undergoing primary GAV. Unusual tissue dissection planes were a risk factor. If injuries were identified intra-operatively, repaired with multilayer closure and evaluated by CRS, patients did well without the development of RVF despite completion of full depth GAV. It is reasonable to complete the full depth vagina, but patients have a significant risk of post-operative vaginal stenosis. SOURCE OF Funding: None